MRSA und Wunden
Werbung

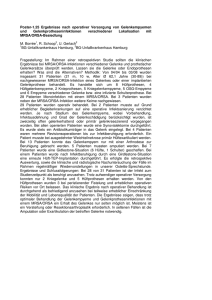
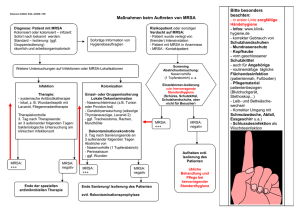
MRSA und Wunden - Einführung in die Thematik - Priv.-Doz. Dr. med. Joachim Dissemond Klinik für Dermatologie, Venerologie und Allergologie Universitätsklinikum Essen Bakteriologischer Abstrich Resistogramm ORSA ≈ MRSA Historie 1926 Entdeckung Penicillin 1941 Klinische Einführung von Penicillin 1945 Penicillin resistenter Staph. aureus 1958 Klinische Einführung von Methicillin 1961 MRSA 1996 VISA (Japan) 1998 VISA (Deutschland) 2002 VRSA (USA) Methicillin-Resistenz Mutation im mecA-Gen kodiert für modifiziertes Penicillinbindungsprotein (PBP) Expression von PBP2a erniedrigte Affinität zu ß-Laktamantibiotika MRSA MRSA Problematik Reinigung / Desinfektion / Materialeinsatz Isolierung von Patienten / Bettensperrung verlängerte Liegedauer (DRG!) erhöhte Mortalität (bei Infektion) … 10 häufigste Vektoren Hygienemaßnahmen Hauptvektor Krankenhauspersonal (Hände!) wichtigste Maßnahme Händedesinfektion! (nach jedem Patientenkontakt, sowie nach Ablegen von Handschuhen und Kittel) MRSA in Europa (2004) MRSA in Deutschland % Staphylococcus aureus Isolate. 25 20 15 10 5 0 1990 1995 1998 2002 Dermatologie Jahr Land MRSA Patienten 2000 Japan 31% (41/135) atopische Dermatitis Akiyama et al. J Dermatol Sci 23:155 2004 Ger 21% (17/79) chronische Wunden Dissemond et al. Hautarzt 55:280 2004 Ger 11% (10/88) entzündliche Dermatosen 9% (5/58) Ulcus cruris venosum 0 (0/83) Basaliom Jappe et al. Acta Derm Venereol 84:181 2004 USA 50% (36/72) Ulcus cruris Valencia et al. J Am Acad Dermatol 50:845 2005 China 2% (1/55) atopische Dermatitis Hon et al. Ann Acad Singapore 34:602 2006 Indien 1,5% (1/68) Pyodermien Patil et al. Indian J Dermatol 72:126 bullöses Erysipel Kasagakis et al. Dermatology 212:31 2006 Griech. 43% (6/14) Fragestellung - eigene Studie Die bakterielle Kolonisation chronischer Wunden? Patienten mit Methicillin/Oxacillin resistetem Staphylococcus aureus (MRSA/ORSA)? Bakterienisolate - absolut Bakterienspezies Staphylococcus aureus Pseudomonas aeruginosa E. coli Proteus mirabilis Enterobacter cloacae Streptococcus Gruppe G Serratia marcescens Proteus vulgaris Enterococcus faecalis Enterobacter intermedius Alcaligenes faecalis Alcaligenes xylosoxidans Stenotrophomonas maltophilia Citrobacter freundii Citrobacter braakii Isolate gesamt Anzahl 56 19 11 4 4 2 2 1 1 1 1 1 1 1 1 106 Bakterienisolate - relativ 4% 2% 1%1% 1%1% 1%1% 1% 1% 2% 4% 10% E. coli Staphylococcus aureus Pseudomonas aeruginosa 52% 18% Resistogramme - MRSA Vancomycin Tetracycline Cotrimoxazol Amikain Clindamycin Gentamicin Erythromycin Cefuroxim Imipenem Ofloxacin Ampicillin Penicillin-G Oxacillin 1 S S S S R R R R R R R R R 2 S S S S S S R R R R R R R 3 S S S R R R R R R R R R R 4 S S S S S S S R R R R R R 5 S S S S S R S R R R R R R 6 S S S S R R R R R R R R R 7 S S I R S R S R R R R R R 8 S S I S S R S R R R R R R 9 10 11 S S S R R S R R S R R S R S R R R R R S R R R R R R R R R R R R R R R R R R R 12 S S R S R R R R R R R R R 13 S S S S R S R R R R R R R 14 S S S S R S R R R R R R R 15 S S S S R S R R R R R R R 16 S S R S S R S R R R R R R 17 S S I S R S R R R R R R R S (%) I (%) 100 0 88,2 0 58,8 18 76,5 0 41,1 0 35,3 0 35,3 0 0 0 0 0 0 0 0 0 0 0 0 0 MRSA 21,5% aller Patienten mit einer chronischen Wunde sind mit MRSA kontaminiert! Dissemond et al. Untersuchungen zur bakteriellen Kolonisation chronischer Wunden in einer universitären dermatologischen Wundambulanz unter besonderer Berücksichtigung von ORSA, Hautarzt 2004 55: 280-288. Infekt Kontamination Kolonisation Spülung Spülung (Antiseptika) Bakterien Wunde kritische Kolonisation lokale Infektion Antiseptika Antiseptika Antiseptika + + (Antibiotika) Antibiotika Therapie systemische Infektion Wundspülung Kochsalzlösung 0,9% Ringer Lösung Antiseptische Lokaltherapie Polihexanid Octenidin Silber Antiseptika - chronische Wunden Obsolete Antiseptika Alkohol Acetat (Essig) Wasserstoffperoxid (H2O2) Natrium Hypochlorit Quecksilber, z. B. Mercuchrom® Farbstoffe, z. B. Gentianviolett, Pyoktanin Ethacridinlactat, z. B. Rivanol Kaliumpermanganat topische Antibiotika, z. B. Gentamycin, Neomycin Umstrittene Antiseptika Triclosan PVP-Jod Therapieoptionen - lokal Nachweis Wirkstoff Applikation (mind. 5 Tage) Mupirocin Octenidin Jodophore 3 x täglich 3 x täglich 3 x täglich Nase 1. Wahl 2. Wahl intakte Haut 1. Wahl Chlorhexidin Polihexanid Octenidin Jodophore 1-3 x täglich 1-3 x täglich 1-3 x täglich 1-3 x täglich chronische Wunde 1. Wahl 1-3 x täglich 1-3 x täglich alle 1-3 Tage 1-3 x täglich alle 3 Tage Polihexanid Octenidin Silber 2. Wahl PVP-Jod Alternativ Biochirurgie Therapieoptionen - systemisch AWMF-Leitlinie 2004 (DDG + ADI) Wirkstoff Dosierung/Tag (mind. 7 - 10 Tage) Vancomycin 2 x 1.000mg i. v. Teicoplanin 1 x 400mg i. v. Linezolid 2 x 600mg p. o., i. v. Quinupristin/Dalfopristin 3 x 7,5mg/kg KG i. v. Cotrimoxazol(*) 2 x 960mg p. o., i. v. Fosfomycin* 3 x 5g i. v. Rifampicin* 2 x 600mg p. o., i. v. Fusidinsäure* 3 x 0,5g p. o., i. v. * nicht als Monotherapie Therapieoptionen - systemisch Antibiotikum Resistenzen (NRZ, 2004) Vancomycin 0 Linezolid 0 Quinupristin/Dalfopristin 0 Teicoplanin 0,1% Rifampicin 2,0% Cotrimoxazol 3,6% Fusidinsäure 4,6% Therapieoptionen - systemisch „Neue“ Antibiotika Wirkstoff Produkt Dosierung/Tag (mind. 1-2 Wochen) Daptomycin Cubicin® 1 x 4 mg/kg KG i. v. Tigecyclin Tygacil® 2 x 50 mg i. v. Therapieoptionen - systemisch Wirkstoff Tagestherapiekosten (€) Vancomycin ~ 70,- Teicoplanin ~ 100,- Linezolid ~ 180,- Quinopristin/Dalfopristin ~ 270,- Cotrimoxazol ~ 2,- Daptomycin ~ 110,- Tigecyclin ~ 125,- Fazit Bis zum Beweis des Gegenteils ist jeder un r h c ea l i s t i s i s l Patient mit einer chronischen Wunde so zu t a i s e r c h n u behandeln als wäre er MRSA positiv ! Zusammenfassung bakteriologische Abstriche entnehmen strikte Umsetzung von Hygienemaßnahmen Sanierung von MRSA-Trägern systemische Antibiose nur bei klinisch manifesten Infektionen (an Resistogramm adaptieren)