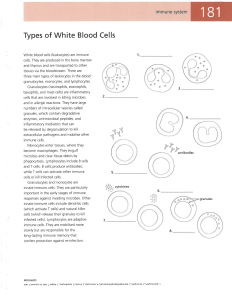
[ Topics in Practice Management ] ICU–Acquired Weakness A Rehabilitation Perspective of Diagnosis, Treatment, and Functional Management Richard D. Zorowitz, MD ICU-acquired weakness (ICUAW) occurs with reported incidence rates from 25% to 100%. Risk factors include immobility, sepsis, persistent systemic inflammation, multiorgan system failure, hyperglycemia, glucocorticoids, and neuromuscular blocking agents. The pathophysiology remains unknown. Clinical features may be neuropathic, myopathic, or a combination of both. Although manual muscle testing is more practical in diagnosing ICUAW, the “gold standard” for the diagnosis of ICUAW remains electromyography and nerve conduction studies. The only potential interventions known to date to prevent ICUAW include insulin therapy and early rehabilitation, but patients still may develop activity limitations in the acute care hospital. For these patients, rehabilitation may continue in long-term care hospitals, inpatient rehabilitation facilities, or skilled nursing facilities. ICUAW is a catastrophic and debilitating condition that potentially leaves patients with permanent residual activity limitations and participation restrictions. Further research on ICUAW needs to better understand its pathophysiology so that more definitive preventive and therapeutic interventions may be developed. KEY WORDS: critical care; myopathy; neuropathy; rehabilitation ICU-acquired weakness (ICUAW) occurs commonly, with reported incidence rates from 25% to 100%.1,2 As opposed to diseases and syndromes directly involving the brain, spinal cord, and peripheral nerves,3 ICUAW is associated with unrelated conditions.4 Its pathophysiology remains unknown. This review presents aspects of ICUAW from a rehabilitation perspective. A more detailed description of the proposed pathophysiology, risk factors, diagnosis, and treatment of ICUAW may be found elsewhere.5 Risk Factors Patients in the ICU may be bedridden and immobile for prolonged periods. For patients ABBREVIATIONS: CIM = critical illness myopathy; CIP = critical illness polyneuropathy; EMG = electromyography; ICUAW = ICU-acquired weakness; IRF = inpatient rehabilitation facility; LTCH = long-term care hospital; RR = risk ratio; SNF = skilled nursing facility AFFILIATIONS: From the MedStar National Rehabilitation Network, Washington, DC. 966 Topics in Practice Management CHEST 2016; 150(4):966-971 requiring mechanical ventilation or prolonged sedation, it is not surprising that a certain amount of weakness occurs. However, ICUAW usually is associated with sepsis, persistent systemic inflammation, and multiorgan system failure.1,4 Approximately 47% to 70% of patients admitted to the ICU for primary sepsis and multiorgan failure may develop electrophysiological evidence of axonal motor-sensory polyneuropathies within 1 to 3 weeks.2,4,6-10 Of these, 35% to 50% have substantial weakness. Women may be as much as four times as likely to develop ICUAW as men, possibly because of their smaller muscle masses.1 CORRESPONDENCE TO: Richard D. Zorowitz, MD, MedStar National Rehabilitation Network, 102 Irving St NW, Room 1321, Washington, DC 20010; e-mail: [email protected] Copyright Ó 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved. DOI: http://dx.doi.org/10.1016/j.chest.2016.06.006 [ 150#4 CHEST OCTOBER 2016 ] Hypoalbuminemia and other nutritional factors also may be involved.4 The role of hyperglycemia11 and glucocorticoid therapy as risk factors of ICUAW is controversial.12-15 Nonetheless, it appears reasonable to minimize the use of glucocorticoids in patients in the ICU, given the known adverse effects of these drugs. The role of neuromuscular blocking agents used in conjunction with glucocorticoids also is controversial; one study in patients with severe ARDS suggested that treatment for less than 48 h might improve survival because of protection of the diaphragm from injury resulting from patient-ventilator dyssynchrony.8,16 Clinical Features Clinical features of ICUAW may be neuropathic, myopathic, or a combination of both.17 Clinical features of each condition, known as critical illness polyneuropathy (CIP) and critical illness myopathy (CIM), are listed in Table 1.18-26 Prevention Medical and rehabilitation interventions may help to prevent ICUAW. In a Cochrane Review of four interventions for preventing CIP and CIM,27 intensive insulin therapy significantly reduced CIP and CIM in the screened (n ¼ 825; risk ratio [RR], 0.65; 95% CI, 0.55-0.77) and total (N ¼ 2,748; RR, 0.70; 95% CI, 0.60-0.82) populations randomized; decreased duration of mechanical ventilation, ICU stay, and 180-day mortality, but did not reduce 30-day mortality when compared with conventional insulin therapy.28,29 Corticosteroids had no effect on treating CIP or CIM or decreasing 180-day mortality, new infections, glycemia at day 7, or episodes of pneumonia, but reduced the incidence of new shock events.30 Early physical therapy reduced the incidence of CIP and CIM in 82 of 104 evaluable participants in the ICU (RR, 0.62; 95% CI, TABLE 1 0.39-0.96), but lost statistical significance in a full intention-to-treat analysis (RR, 0.81; 95% CI, 0.60-1.08).31 The duration of mechanical ventilation but not ICU stay was significantly shorter in the intervention group. Hospital mortality was not affected, but 30- and 180-day mortality results were not available. Finally, electrical muscle stimulation given to 52 evaluable subjects of 140 did not significantly reduce the incidence of CIP and CIM when compared with no stimulation (RR, 0.32; 95% CI, 0.10-1.01) as well as in an intention-to-treat analysis (RR, 0.94; 95% CI, 0.78-1.15).32 There was no effect on duration of mechanical ventilation or ICU mortality, and 30- and 180-day mortality were not reported. The data also were prone to bias because of imbalances between treatment groups in the subgroup of participants. A separate systematic review and meta-analysis of physical therapy in the ICU demonstrated significant positive effects on quality of life (g ¼ 0.40; 95% CI, 0.08-0.71), physical function (g ¼ 0.46; 95% CI, 0.13-0.78), peripheral muscle strength (g ¼ 0.27; 95% CI, 0.02-0.52), respiratory muscle strength (g ¼ 0.51; 95% CI, 0.12-0.89), and ventilator-free days (g ¼ 0.38; 95% CI, 0.16-0.59); and significant decreases in length of hospital stay (g ¼ –0.34; 95% CI, –0.53 to –0.15) and ICU stay (g ¼ –0.34; 95% CI, –0.51 to –0.18).33 There was no effect on mortality. Diagnosis Given the clinical features of ICUAW (Table 1), it would be simple to use manual muscle strength to identify the distribution and degree of muscle weakness; however, only approximately to 25% to 29% of patients are adequately awake to assess muscle strength.1,34 Therefore, more accurate methods of assessing muscle weakness are needed. The “gold standard” for the diagnosis of ICUAW remains electromyography (EMG). In CIP, electrophysiological changes can be detected as early as 24 to 48 h following the onset of ICUAW, and often ] Clinical Features of ICUAW Feature Weakness Muscle atrophy Ventilatory failure CIP Flaccid Worse distally more than proximally CIM Flaccid Worse proximally more than distally () () () () Muscle stretch reflexes Hyporeflexia or areflexia Normal or hyporeflexia Sensory loss May experience distal sensory loss18,19 Normal Extraocular muscles (-) Rare, although facial weakness may occur CIM ¼ critical illness myopathy; CIP ¼ critical illness polyneuropathy; ICUAW ¼ ICU-acquired weakness. journal.publications.chestnet.org 967 precede clinical findings.35 EMG characteristics of CIP and CIM are listed in Table 2.36 Because EMG requires some participation of the patient, the use of peroneal and sural nerve conduction studies show promise as accurate screens for ICUAW and may assist in determining which patients need further EMG studies to confirm a diagnosis.37 Prognosis Rehabilitation Because of the increase in patients with activity limitations resulting from ICUAW, the paradigm of treatment has shifted from the liberal use of sedation and immobilization to mobilization.43 The first study of ICU rehabilitation given to mechanically ventilated patients demonstrated not only that activity was feasible and safe, but also that patients ambulated a mean distance of 212 feet by the time of discharge from the ICU44; however, research is needed to definitively evaluate safety and long-term benefits of ICU mobilization. Technology and improved medical management has resulted in a dramatic increase in patients with ICUAW.38,39 Up to 65% of patients who require prolonged mechanical ventilation have activity limitations when they are discharged from the hospital.7,31 In older survivors of ICUAW, activity limitations persisted 1 year after discharge.40 Muscle weakness and activity limitations frequently were observed in ARDS survivors after 1 year, and even after 5 years, 6-min walk tests scores were only 70% of predicted results.38 Although CIM is associated with a higher rate of recovery than CIP,17 neuromuscular impairment may last as long as 15 years with either condition.41 In addition to issues with mobility, nutrition also needs to be addressed. In one small study of patients with ICUAW transferred to a long-term care hospital (LTCH), anemia, hypoalbuminemia, and vitamin D deficiency were identified, as were impairments in strength, balance, coordination, mobility, and endurance.45 These findings emphasize the need for an interdisciplinary team of health professionals, including occupational therapy for feeding, speech-language pathology for swallowing, and a nutritionist for dietary guidance. Electrophysiological studies also may provide clues to the prognosis of ICUAW. A reduced CMAP on the eighth day of ICU admission carried a high negative predictive value for weakness after 1 year, but was associated with a higher 1-year mortality rate.42 However, an abnormal sensory nerve action potential and the presence of fibrillation potentials on the 15th day of ICU admission carried a high positive predictive value for weakness. Nonetheless, patients with ICUAW may require rehabilitation in and beyond the acute care hospital. Early consultation with physical therapy, occupational therapy, speech-language pathology, and/or rehabilitation physicians is essential to prevent complications from immobilization, decrease activity limitations, and prepare patients for discharge from the acute care hospital. A randomized pilot study of 12 weeks of intensive telerehabilitation vs conventional TABLE 2 ] EMG Characteristics of ICUAW Characteristic CMAP CIP Low amplitude CIM At least 1 low amplitude Variable duration Sensory nerve action potentials Low amplitude or absent Normal dmCMAP Low Low Nerve-evoked CMAP-to-dmCMAP ratio < 0.5 > 0.5 Fibrillation potentials (reflect denervation) Found in distal and proximal muscles in multifocal pattern with variable severity May be found in 30% of diaphragm Found in at least 1 muscle in 71% to 100% of patients May be diffuse Motor unit recruitment Decreased Early and full May be of short duration and low amplitude Modified from Lacomis D.36 CMAP ¼ compound muscle action potentials; dmCMAP ¼ direct muscle CMAP; EMG ¼ electromyography. See Table 1 legend for expansion of other abbreviations. 968 Topics in Practice Management [ 150#4 CHEST OCTOBER 2016 ] care in general medical or surgical ICU survivors with either cognitive or functional impairment demonstrates promise in improving cognitive performance and functional outcomes.46 However, patients who cannot return home when they are ready for discharge may be referred for postacute rehabilitation to LTCHs, inpatient rehabilitation facilities (IRF), or skilled nursing facilities (SNF). Currently, no definitive studies have evaluated the effects of rehabilitation programs in inpatient or outpatient settings on this population. Availability and quality of these facilities may be limited geographically and may affect the medical and functional management of the patient. Under Medicare guidelines, an LTCH treats medically complex patients who require long-stay hospital-level care, and has an average inpatient length of stay greater than 25 days. An LTCH must provide complex respiratory services and complex wound services; 24/7 physician on-site or on-call coverage; 24/7 registered nurse–level nursing; 24/7 advanced cardiac life support; and 24/7 availability of respiratory therapists. Patients meet Medicare criteria for LTCH admission immediately following discharge from an acute care hospital that included either at least 3 days in an ICU or assignment to a Medicare Severity Long-Term Care Diagnosis Related Group based on the receipt of ventilator services of at least 96 h. Patients cannot have a principal psychiatric or rehabilitation diagnosis, but must have at least two active secondary diagnoses. So, although patients with ICUAW may receive physical therapy, occupational therapy, and/or speech-language pathology, the primary reason for admission usually involves weaning from the mechanical ventilator and decannulation of the tracheostomy. In one study performed in a long-term acute care hospital, a group receiving rehabilitation (n ¼ 18), motor (except for the walking/wheelchair subitem), and cognitive scores of the Functional Independence Measure increased significantly 6 months postenrollment when compared with that of a control group (n ¼ 16).47 The rehabilitation group was completely independent in eating, comprehension, expression, and social interaction. The 1-year survival rate in the rehabilitation group was 70%, compared with 25% of the control group (25%), although the proportion of patients discharged and who were ventilator-free in did not differ significantly between groups. An IRF provides active, ongoing, and intensive therapy involving a coordinated interdisciplinary team approach to physical therapy, occupational therapy, journal.publications.chestnet.org speech-language pathology, or prosthetics/orthotics, of which at least one therapy must include physical or occupational therapy. Under Medicare guidelines, patients admitted to an IRF must require, actively participate in, benefit significantly from, and make measurable improvement from at least 3 h of therapy per day at least 5 days per week, or in certain welldocumented cases, at least 15 h of therapy within consecutive 7-day periods. A rehabilitation physician must visit the patients face-to-face at least 3 days per week to assess and modify the course of medical and functional treatment. Some IRFs can manage patients on mechanical ventilators or with tracheostomies while providing therapy. In these cases, patients are admitted because of activity limitations resulting from ICUAW. The rehabilitation team is depicted in Figure 1. Admission to a SNF may be considered if patients need inpatient rehabilitation care but do not meet the criteria for admission to an LTCH or IRF. Under Medicare guidelines, patients must be transferred to a SNF within 30 days after discharge from a medically necessary stay of at least 3 consecutive calendar days in the hospital and treated for a condition that was treated during the qualifying hospital stay or for a condition that arose while in the SNF. Under certain alternative payment models, the 3-day requirement may be waived by a medical director. Nursing care is provided by or under the supervision of a registered professional nurse. Physical therapy, occupational therapy, and/or speech-language pathology services are furnished by the SNF or under arrangements with another entity. Patients may receive up to 3 h of therapies daily up to 5 days per week. The SNF is responsible for the cost of drugs, biologicals, supplies, appliances, and equipment that are required for the care and treatment of their patients. Nurse Physician Neuropsychology Family, Friends, and Caregivers Nutritionist PATIENT Recreational Therapy Social Worker / Case Manager Physical Therapy Occupational Therapy Speech-Language Pathology Figure 1 – The rehabilitation team. Health-care professionals work in a coordinated fashion toward a common goal for the patient, the center of care. 969 Patients with ICUAW usually do not receive rehabilitation in one level of care. One study demonstrated that, on average, patients transferred almost five times among acute care hospitals, LTCHs, IRFs, SNFs, and home care during the first year of treatment.48 These data emphasize that patients wax and wane medically and functionally during their course of recovery; thus, it is not surprising that the costs of treatment for patients with ICUAW usually are substantial. 11. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19): 1359-1367. Conclusion 15. Hermans G, Wilmer A, Meersseman W, et al. Impact of intensive insulin therapy on neuromuscular complications and ventilator dependency in the medical intensive care unit. Am J Respir Crit Care Med. 2007;175(5):480-489. In summary, ICUAW occurs commonly. Although there are many risk factors, the pathophysiology remains unknown. Clinical features may be neuropathic, myopathic, or a combination of both. The “gold standard” for the diagnosis of ICUAW remains EMG. There are several postacute rehabilitation options if the patient cannot be discharged home from the acute care hospital. Patients may have activity limitations for many years after onset. Until more definitive preventative and therapeutic interventions are identified, it is important to keep patients as mobile in the ICU as possible, so that they do not fall victim to this catastrophic and debilitating condition. Acknowledgments Financial/nonfinancial disclosures: None declared. References 1. De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288(22):2859-2867. 2. Bednarík J, Vondracek P, Dusek L, Moravcova E, Cundrle I. Risk factors for critical illness polyneuromyopathy. J Neurol. 2005;252(3): 343-351. 3. Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. N Engl J Med. 2014;370(17):1626-1635. 4. Druschky A, Herkert M, Radespiel-Troger M, et al. Critical illness polyneuropathy: clinical findings and cell culture assay of neurotoxicity assessed by a prospective study. Intens Care Med. 2001;27(4):686-693. 5. Jolley SE, Bunnell A, Hough CL. Intensive care unit acquired weakness [published online ahead of print April 7, 2016]. Chest. http://dx.doi.org/10.1016/j.chest.2016.03.045. 6. Dock W. The evil sequelae of complete bed rest. JAMA. 1944;125(16): 1083-1085. 7. Herridge MS, Cheung AM, Tansey CM, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;348(8):683-693. 8. Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107-1116. 9. Griffiths RD, Palmer TE, Helliwell T, MacLennan P, MacMillan RR. Effect of passive stretching on the wasting of muscle in the critically ill. Nutrition. 1995;11(5):428-432. 10. Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794. 970 Topics in Practice Management 12. Derde S, Hermans G, Derese I, et al. Muscle atrophy and preferential loss of myosin in prolonged critically ill patients. Crit Care Med. 2012;40(1):79-89. 13. van den Berghe G, Schoonheydt K, Becx P, Bruyninckx F, Wouters PJ. Insulin therapy protects the central and peripheral nervous system of intensive care patients. Neurology. 2005;64(8): 1348-1353. 14. Garnacho-Montero J, Madrazo-Osuna J, Garcia-Garmendia JL, et al. Critical illness polyneuropathy: risk factors and clinical consequences: a cohort study in septic patients. Intens Care Med. 2001;27(8):1288-1296. 16. Leatherman JW, Fluegel WL, David WS, Davies SF, Iber C. Muscle weakness in mechanically ventilated patients with severe asthma. Am J Respir Crit Care Med. 1996;153(5):1686-1690. 17. Koch S, Spuler S, Deja M, et al. Critical illness myopathy is frequent: accompanying neuropathy protracts ICU discharge. J Neurol Neurosurg Psychiatry. 2011;82:287-293. 18. Zifko UA, Zipko HT, Bolton CF. Clinical and electrophysiological findings in critical illness polyneuropathy. J Neurol Sci. 1998;159(2): 186-193. 19. de Seze M, Petit H, Wiart L, et al. Critical illness polyneuropathy. A 2-year follow-up study in 19 cases. Eur Neurol. 2000;43(2):61-69. 20. Douglass JA, Tuxen DV, Horne M, et al. Myopathy in severe asthma. Am Rev Respir Dis. 1992;146(2):517-519. 21. Campellone JV, Lacomis D, Kramer DJ, Van Cott AC, Giuliani MJ. Acute myopathy after liver transplantation. Neurology. 1998;50(1): 46-53. 22. Blackie JD, Gibson P, Murree-Allen K, Saul WP. Acute myopathy in status asthmaticus. Clin Exp Neurol. 1992;30:72-81. 23. Griffin D, Fairman N, Coursin D, Rawsthorne L, Grossman JE. Acute myopathy during treatment of status asthmaticus with corticosteroids and steroidal muscle relaxants. Chest. 1992;102(2): 510-514. 24. Lacomis D, Giuliani MJ, Van Cott A, Kramer DJ. Acute myopathy of intensive care: clinical, electromyographic, and pathological aspects. Ann Neurol. 1996;40(4):645-654. 25. Sitwell LD, Weinshenker BG, Monpetit V, Reid D. Complete ophthalmoplegia as a complication of acute corticosteroid- and pancuronium-associated myopathy. Neurology. 1991;41(6):921-922. 26. Shee CD. Risk factors for hydrocortisone myopathy in acute severe asthma. Respir Med. 1990;84(3):229-233. 27. Hermans G, De Jonghe B, Bruyninckx F, Van den Berghe G. Interventions for preventing critical illness polyneuropathy and critical illness myopathy. Cochrane Database Syst Rev. 2014;(1): CD006832. 28. Hermans G, Wilmer A, Meersseman W, et al. Impact of intensive insulin therapy on neuromuscular complications and ventilatordependency in MICU. Am J Resp Crit Care Med. 2007;175(5): 480-489. 29. Van den Berghe G, Schoonheydt K, Becx P, Bruyninckx F, Wouters PJ. Insulin therapy protects the central and peripheral nervous system of intensive care patients. Neurology. 2005;64(8): 1348-1353. 30. Steinberg KP, Hudson LD, Goodman RB, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006;354(16):1671-1684. 31. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678): 1874-1882. [ 150#4 CHEST OCTOBER 2016 ] 32. Routsi C, Gerovasili V, Vasileiadis I, et al. Electrical muscle stimulation prevents critical illness polyneuromyopathy: a randomized parallel intervention trial. Crit Care. 2010;14(2):R74. 33. Kayambu G, Boots R, Paratz J. Physical therapy for the critically ill in the ICU: a systematic review and meta-analysis. Crit Care Med. 2013;41(6):1543-1554. 34. Hough CL, Lieu BK, Caldwell ES. Manual muscle strength testing of critically ill patients: feasibility and interobserver agreement. Crit Care. 2011;15(1):1. 35. Khan J, Harrison TB, Rich MM, Moss M. Early development of critical illness myopathy and neuropathy in patients with severe sepsis. Neurology. 2006;67(8):1421-1425. 36. Lacomis D. Electrophysiology of neuromuscular disorders in critical illness. Muscle Nerve. 2013;47(3):452-463. 37. Moss M, Yang M, Macht M, et al. Screening for critical illness polyneuromyopathy with single nerve conduction studies. Intens Care Med. 2014;40(5):683-690. 38. Herridge MS, Tansey CM, Matt A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293-1304. 41. Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med. 2011;39(2):371-379. 42. Hermans G, Van Mechelen H, Bruyninckx F, et al. Predictive value for weakness and 1-year mortality of screening electrophysiology tests in the ICU. Intens Care Med. 2015;41(12):2138-2148. 43. Needham DM. Mobilizing patients in the intensive care unit: improving neuromuscular weakness and physical function. JAMA. 2008;300(14):1685-1690. 44. Stiller K, Phillips AC, Lambert P. The safety of mobilisation and its effects on haemodynamic and respiratory status of intensive care patients. Physiother Theory Pract. 2004;20(3):175-185. 45. Wells C, Steinbrenner G, Beans J, et al. Severe immobility and malnutrition in post ICU patients requiring prolonged mechanical ventilation: an unmet rehabilitation need. Am J Respir Crit Care Med. 2012;185:A6852. 46. Jackson J, Ely EW, Morey MC, et al. Cognitive and physical rehabilitation of ICU survivors: results of the RETURN randomized, controlled pilot investigation. Crit Care Med. 2012;40(4):1088-1097. 39. Hopkins RO, Jackson JC. Short- and long-term cognitive outcomes in intensive care unit survivors. Clin Chest Med. 2009;30(1):143-153. 47. Chen S, Su CL, Wu YT, et al. Physical training is beneficial to functional status and survival in patients with prolonged mechanical ventilation. J Formos Med Assoc. 2011;110(9):572-579. 40. Sacanella E, Perez-Castejon JM, Nicolas JM, et al. Functional status and quality of life 12 months after discharge from a medical ICU in healthy elderly patients: a prospective observational study. Crit Care. 2011;15(2):1. 48. Unroe M, Kahn JM, Carson SS, et al. One-year trajectories of care and resource utilization for recipients of prolonged mechanical ventilation: a cohort study. Ann Intern Med. 2010;153(3):167-175. journal.publications.chestnet.org 971