Mutationen im MFN2-Gen als Ursache der hereditären peripheren
Werbung

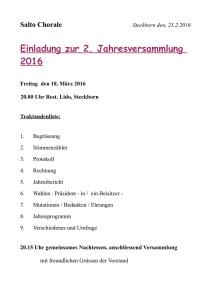
Ruhr-Universität Bochum PD Dr. med. Moritz Meins Dienstort: Ärztliche Partnerschaft Wagner Stibbe Göttingen Mutationen im MFN2-Gen als Ursache der hereditären peripheren Polyneuropathie Charcot-Marie-Tooth Typ 2 Kumulative Inaugural-Dissertation zur Erlangung des Doktorgrades der Medizin einer Hohen Medizinischen Fakultät der Ruhr-Universität Bochum vorgelegt von Kathrin Engelfried aus Esslingen (am Neckar) 2007 Dekan: Prof. Dr. med. G. Muhr Referent: PD Dr. med. M. Meins Korreferent: Prof. Dr. med. M. Vorgerd Tag der mündlichen Prüfung: 17. 06. 2008 Für meine Familie Inhaltsverzeichnis -I- Inhaltsverzeichnis Abkürzungsverzeichnis ................................................................................... II Tabellenverzeichnis ........................................................................................ IV Abbildungsverzeichnis ................................................................................... IV 1 Einleitung................................................................................................... 1 1.1 Charcot-Marie-Tooth Neuropathien (CMT) ...................................... 1 1.1.1 Elektrophysiologische und histopathologische Einteilung............. 2 1.1.2 Molekulargenetik der CMT............................................................ 4 1.2 Physiologie und Pathophysiologie der Mitochondrien .................. 6 1.2.1 Das MFN2-Gen............................................................................. 7 1.2.2 Aufbau, Lokalisation und Funktion des MFN2-Proteins ................ 8 2 Zielsetzung der Arbeit ............................................................................ 10 3 Methode und Ergebnisse ....................................................................... 11 3.1 Mutationsanalyse des MFN2-Gens................................................. 11 3.2 Ergebnisse ....................................................................................... 11 4 Diskussion............................................................................................... 14 5 Literaturverzeichnis ................................................................................ 17 6 Danksagung ............................................................................................ 24 7 Lebenslauf ............................................................................................... 25 8 Veröffentlichung ..................................................................................... 27 Abkürzungsverzeichnis Abkürzungsverzeichnis AS Aminosäure ATP Adenosintriphosphat bp Basenpaare C- Carboxy- Cc coiled-coil CMT Charcot-Marie-Tooth Neuropathie CMT1 Charcot-Marie-Tooth Neuropathie Typ 1 CMT2 Charcot-Marie-Tooth Neuropathie Typ 2 Da Dalton del Deletion DNA desoxyribonucleic acid, Desoxyribonukleinsäure EGR2 Early-Growth-Response-2-Gen et al. und andere F Frau fzo fuzzy onions GARS Glycyl-tRNA-Synthetase-Gen GDAP1 Ganglioside-Induced-Differentiation-Associated-Protein-Gen GJB1 Gap-Junction-Protein-Beta1-Gen GTPase Guanosintriphosphatase HR1 heptad repeat regions 1 HR2 heptad repeat regions 2 HMSN Hereditäre Motorisch-Sensorische Neuropathie HMSN V Hereditäre Motorisch-Sensorische Neuropathie Typ V HMSN VI Hereditäre Motorisch-Sensorische Neuropathie Typ VI HSPB1 Heat-Shock-27kDa-Protein-1-Gen ins Insertion k Kilo kb Kilobasenpaare KIF1B Kinesin-Family-Member-1B-Gen LMNA Lamin-A/C-Gen LITAF Lipopolysaccharide-Induced-TNF-Factor-Gen M Mann MFN1 Mitofusin 1-Gen MFN1 Mitofusin 1-Protein MFN2 Mitofusin 2-Gen -II- Abkürzungsverzeichnis MFN2 Mitofusin 2-Protein mNLG motorische Nervenleitgeschwindigkeit MPZ Myelin-Protein-Zero-Gen mtDNA mitochondriale DNA NEFL Neurofilament-Light-Polypeptide-Gen NLG Nervenleitgeschwindigkeit m/s Meter pro Sekunde N- Amino- OPA1 Optic-Atroph-1-Gen PCR polymerase chain reaction, Polymerasekettenreaktion p kurzer Arm eines Chromosoms; pico (10-12) PMP22 Peripheral-Myelin-Protein-22-Gen q langer Arm eines Chromosoms RAB7 Ras-Associated-Protein-7-Gen SSCP single strand conformation polymorphism SNPs single nucleotide polymorphisms TM Transmembran Nukleobasen/Nukleotide: A Adenin/Adenosin C Cytosin/Cytidin G Guanin/Guanidin T Thymin/Thymidin U Uracil/Uridin P Purin Y Pyrimidin N beliebige(s) Nukleobase/Nukleotid -III- Abkürzungsverzeichnis -IV- Aminosäuren: A Ala Alanin M Met Methionin C Cys Cystein N Asn Asparagin D Asp Asparaginsäure P Pro Prolin E Glu Glutaminsäure Q Gln Glutamin F Phe Phenylalanin R Arg Arginin G Gly Glycin S Ser Serin H His Histidin T Thr Threonin I Ile Isoleucin V Val Valin K Lys Lysin W Trp Tryptophan L Leu Leucin Y Tyr Tyrosin Tabellen- und Abbildungsverzeichnis Tabellenverzeichnis Tab. 1: ................................................................................................................ 4 Tab. 2: ................................................................................................................ 5 Tab. 3: .............................................................................................................. 13 Tab. 4: .............................................................................................................. 13 Abbildungsverzeichnis Abb. 1 ................................................................................................................. 1 Abb. 2 ................................................................................................................. 2 Abb. 3 ................................................................................................................. 7 Abb. 4 ................................................................................................................. 8 Abb. 5 ............................................................................................................... 12 Einleitung 1 1 Einleitung 1.1 Charcot-Marie-Tooth Neuropathien (CMT) Unter Charcot-Marie-Tooth Neuropathien (CMT), auch bekannt unter der Bezeichnung Hereditäre Motorisch-Sensorische Neuropathien (HMSN), versteht man eine Gruppe von genetisch heterogenen Erkrankungen des peripheren Nervensystems. Die CMT zählen mit einer Prävalenz von etwa 1/2500 zu den häufigsten vererbbaren Erkrankungen des Nervensystems [49]. Die Erkrankungen, die nach ihren Entdeckern Jean-Martin Charcot, Pierre Marie und Howard Tooth benannt sind, wurden erstmals 1886 dokumentiert. Die Hauptsymptome sind progressive symmetrisch ausgeprägte Paresen mit distalem Beginn, welche hauptsächlich die Beine, besonders die kleinen Fußmuskeln und die peronealen Muskeln betreffen. Die Muskeleigenreflexe der Beine fehlen oft bereits im frühen Stadium der Erkrankung. Charakteristisch sind Steppergang und Storchenbeine sowie Hohlfüße (Pes cavus) mit Krallenzehen. Abb. 1 CMT2 Patient mit Areflexie und Paresen sowie peroneal betonter Atrophie der Beine. (Mit freundlicher Genehmigung von Herrn Prof. Dr. med. M. Vorgerd) Einleitung 2 Die Ursache der Paresen liegt in einer durch Neuropathie bedingten Unterversorgung der Muskulatur mit Nervenimpulsen. Trotz Bewegung tritt ein Abbau der Muskulatur ein. Dieser Vorgang wird als neurogene Muskelatrophie bezeichnet. Es kommt zunehmend zum Verlust der motorischen und sensorischen Fähigkeiten. Abb. 2 Deutlich ausgeprägte Fußheberschwäche bei einem CMT2 Patienten. (Mit freundlicher Genehmigung von Herrn Prof. Dr. med. M. Vorgerd) 1.1.1 Elektrophysiologische und histopathologische Einteilung Die CMT lässt sich nach neurophysiologischen und histopathologischen Kriterien in zwei Typen unterteilen [18]. Die meisten Patienten können entweder zur demyelinisierenden CMT1 mit starker Verminderung der motorischen Nervenleitgeschwindigkeit (mNLG) unter 38 m/s oder zur axonalen (neuronalen) CMT2 mit mäßig verminderter oder normaler mNLG von über 38 m/s gezählt werden [24]. In einigen CMT-Familien bestehen allerdings Schwierigkeiten, die Erkrankung nach strengen neurophysiologischen Kriterien in eine der beiden Kategorien einzuordnen. Zunehmend wird in der Literatur deshalb von einem intermediärem Typ gesprochen. Die mNLG des Nervus medianus liegt in diesen Fällen im Bereich von 25 bis 45 m/s [14]. Einleitung 3 Dem neurophysiologischen Befund entsprechend findet sich bei der CMT1 als histologisches Korrelat eine Demyelinisierung der Markscheide. Durch wiederholte De- und Remyelinisierung der Nerven bilden sich histopathologisch ein nachweisbarer segmentaler Markscheidenzerfall und sogenannte Zwiebelschalenformationen aus [55]. Bei Patienten mit CMT2 findet sich histologisch primär weder Markscheidenzerfall noch Zwiebelschalenformation. Morphologisch dominiert der Verlust von großen myelinisierten Axonen. Es lassen sich Zeichen der Regeneration mit einer großen Anzahl an kleinen dünnen myelinisierten Axonen finden [55]. Die NLG ist meist normal oder nur geringfügig erniedrigt. Die Amplitude der motorischen und sensorischen Aktionspotentiale ist jedoch erniedrigt [24]. Manche Familien mit CMT-Neuropathien zeigen zusätzlich zu den bereits genannten Hauptsymptomen noch eine große Variation begleitender Symptome. Auch der Erbgang der CMT ist nicht einheitlich: In vielen Familien ist eine autosomal–dominante Vererbung der CMT zu erkennen. Es gibt jedoch auch Familien mit autosomal-rezessiver oder geschlechtsgebundener (X-chromosomaler) Vererbung. Deshalb wurde neben der Einteilung in die Hauptformen CMT1 und CMT2 noch eine Abgrenzung weiterer Unterformen vorgenommen [35]. Weiterhin ist auch eine Subklassifizierung der CMT1 und der CMT2 erfolgt. Die Unterscheidung dieser Subtypen ist in den meisten Fällen darin begründet, dass Mutationen in unterschiedlichen Genen mit unterschiedlicher chromosomaler Lokalisation zur Ausprägung einer CMT1 bzw. CMT2 führen. Die Zuordnung eines Patienten oder einer Familie zu einem bestimmten Subtyp ist einerseits durch den Nachweis der ursächlichen Mutation in einem bestimmten CMTKrankheitsgen, durch Familienuntersuchungen (Kopplungsanalysen) oder durch zusätzliche, für einen bestimmten CMT-Subtyp spezifische Symptome möglich. Auf folgender Internetseite kann eine ständig aktualisierte Mutationsdatenbank der CMT1- und CMT2-Erkrankungen mit begleitenden Symptomen eingesehen werden: http://www.molgen.ua.ac.be/CMTMutations. Unter anderem werden Symptome wie spastische Paresen, Optikusatrophie, Neuropathien der Hirnnerven, Glaukom und Neutropenie beobachtet [64]. Beispielsweise wird die CMT2 mit Optikusatrophie als HMSN VI subklassifiziert [8] und die CMT2 mit Pyramidenbahnzeichen ist auch als HMSN V bekannt [25]. Einleitung 4 Ein Überblick über die genetische Klassifikation der CMT1 und der CMT2 kann den Tabellen 1 und 2 entnommen werden. Auf eine Auflistung der klinischen Symptome wurde verzichtet. Es wird an dieser Stelle auf die einschlägige klinische Literatur verwiesen. 1.1.2 Molekulargenetik der CMT Molekulargenetische Studien haben sowohl für CMT1 als auch für CMT2 genetische Heterogenität und Polygenie bewiesen. Patienten mit identischem Phänotyp können Mutationen in unterschiedlichen Genen aufweisen. Andererseits können auch Mutationen im gleichen Gen zu unterschiedlichen Phänotypen führen [7, 59]. Im Vergleich zur CMT1, deren krankheitswirksame genetische Defekte gut untersucht sind, wurden Gene, welche der CMT2-Erkrankung zugrunde liegen, erst in der letzten Zeit identifiziert [52]. Tab. 1: Genetische Klassifikation der CMT1 [9, 31] Genetische Klassifikation Gen Abkürzung Lokalisation des Gens CMT1A PeripheralMyelin-Protein-22Gen (Duplikation) PMP22 Chromosom 17p11.2 [37, 45, 58] CMT1B Myelin-ProteinZero-Gen MPZ, P0 Chromosom 1q22-q23 [26] CMT1C Lipopolysaccharide-Induced-TNFFactor-Gen LITAF Chromosom 16p13.13 [51] CMT1D Early-GrowthResponse-2-Gen EGR2 Chromosom 10q21-q22 [61] CMT1E Peripheral-MyelinProtein-2-Gen (Punktmutationen) PMP22 Chromosom 17p11.2 [57] CMT 1F/2E NeurofilamentLight-PolypeptidGen NEFL Chromosom 8p21 [30] Literaturverweis Einleitung 5 Tab. 2: Genetische Klassifikation der CMT2 [10, 31] Genetische Klassifikation Gen Abkürzung des Gens Mitofusin 2-Gen MFN2 Kinesin-FamilyMember-1B-Gen KIF1B CMT2B Ras-AssociatedProtein-7-Gen CMT2B1 Lokalisation Literaturverweis Chromosom 1p35-p36 [65] [62] RAB7 Chromosom 3q21 [60] Lamin A/C-Gen LMNA Chromosom 1q21.2-q21.3 [16] CMT2B2 Gen nicht identifiziert Gen nicht identifiziert Chromosom 19q13.3 [6] CMT2C (HMSN IIC) Gen nicht identifiziert Gen nicht identifiziert Chromosom 12q23-24 [33] CMT2D Glycyl-tRNASynthetase-Gen GARS Chromosom 7p15 [2] CMT2E/1F NeurofilamentLight-PolypeptideGen NEFL Chromosom 8p21 [39] CMT2F Heat-Shock27kDa-Protein-1Gen HSPB1 Chromosom 7q11.23 [21] CMT2G Gen nicht identifiziert Gen nicht identifiziert Chromosom 12q12-13.3 [40] CMT2H Gen nicht identifiziert Gen nicht identifiziert Chromosom 8q21 [4] CMT2I Myelin-ProteinZero-Gen MPZ, P0 Chromosom 1q22-q23 [38] CMT2J Myelin-ProteinZero-Gen MPZ, P0 Chromosom 1q22-q23 [15] CMT2K, CMT4A Ganglioside -InducedDifferentiationAssociated-Protein –1-Gen GDAP1 Chromosom 8q21.1 [13] CMT2L Gen nicht identifiziert Gen nicht identifiziert Chromosom 12q24 [53] CMTX, CMTX1 Gap-JunctionProtein-Beta1-Gen GJB1, Co32 Chromosom Xq13.1 [56] HMSN V HMSN VI Mitofusin 2-Gen MFN2 Chromosom 1p35-p36 [63, 64] CMT2A Einleitung 6 Das mutierte Gen Mitofusin 2 (MFN2), welches in dieser Arbeit untersucht wurde, wird für die Entstehung der CMT2A verantwortlich gemacht [5, 65]. Zhao et al. beschrieb eine Mutation im Kinesin-Family-Member-1B-Gen (KIF1B) in einer großen CMT2A Familie [62]. Jedoch wurden bis jetzt keine weiteren Mutationen im KIF1B-Gen entdeckt, welche in Zusammenhang mit CMT2A Patienten stehen. 2004 gelang es Züchner et al. erstmalig, in sieben großen CMT2A Familien mittels Kopplungsanalysen zahlreiche Mutationen im MFN2-Gen zu lokalisieren [65]. Zwischenzeitlich wurden ebenfalls von anderen Arbeitsgruppen Mutationen im MFN2-Gen, die mit CMT2A assoziiert sind, beschrieben [19, 32, 36, 63, 64]. 1.2 Physiologie und Pathophysiologie der Mitochondrien In der Mitte des 19. Jahrhunderts entdeckte Flemming Mitochondrien als anfärbbare Granula im Zytoplasma. Sie nehmen eine zentrale Position im zellulären Metabolismus und in energiegewinnenden Prozessen ein. Diese Energie benötigt die Zelle zum Wachstum, zur Differenzierung und zur Biogenese von Organellen. Sie wird durch den Zitratzyklus, die oxidative Phosphorylierung und schließlich durch die ATP-Synthese geliefert. Mitochondrien sind auch an weiteren Prozessen wie Fettsäureabbau, Hämbiosynthese und der Biosynthese von Eisen-Schwefel-Komplexen beteiligt [46]. Mitochondrien formen dynamische, netzwerkartige Strukturen, die durch ständige Teilungs- und Fusionsprozesse aufrecht erhalten werden [43]. Dabei können diese Organellen ihre Anzahl, Form und Proteinkomposition auf unterschiedlichste metabolische Differenzierungsstadien einstellen [48]. In Hepatozyten oder Fibroblasten finden sich längliche Mitochondrien mit einer Länge von rund 4 µm. In einigen Zelltypen wie z.B. Muskelzellen mit hohem Energiebedarf nehmen die Mitochondrien über 30% des Zellvolumens ein. Sie bilden Netzwerke aus und ordnen sich entlang der energieverbrauchenden Strukturen an [3]. Die Ausbildung umfangreicher mitochondrialer Netzwerke innerhalb der Zelle stellt einen wichtigen Beitrag zur Sicherstellung der Energieversorgung in den Zellkompartimenten dar [50]. Untersuchungen an Synapsen haben gezeigt, dass es in diesen Strukturen zu einer bemerkenswert großen Einleitung 7 Ansammlung an Mitochondrien kommt [44]. Ist die Ausbildung von Netzwerken gestört und der Transport entlang des Axons über eine relativ große Distanz nicht möglich, so kann die Funktion des peripheren Nervs nicht aufrecht erhalten werden. Die Folge ist axonale Degeneration. Die Prävalenz neuronaler Erkrankungen, welche mit Mutationen in mitochondrialen Genen assoziiert sind, zeigt die große Bedeutung der Mitochondrien für die Neuronen. So weisen beispielsweise mitochondriale Enzephalomyopathien, welche durch Mutationen der mitochondrialen DNA (mtDNA) verursacht sind, oft charakteristische neurologische Symptome auf [17, 54]. Mutationen im Paraplegin-Gen, das eine ATPase in der inneren Mitochondrienmembran kodiert, verursachen eine Form der Hereditären Spastischen Paraplegie (HSP). Tierexperimente an Mäusen zeigen abnormale Mitochondrienstrukturen bevor es zu einer axonalen Degeneration kommt [22]. Auch bei CMT2-Patienten ist die mitochondriale Funktion gestört. Nur wenige Informationen über die Histopathologie der Mitochondrien in CMT2-Patienten sind bis jetzt bekannt. Ebenso unklar ist, welche mitochondrialen Dysfunktionen genau vorliegen [11]. Weitere Studien werden nötig sein, um neue Erkenntnisse über mitochondriale und zelluläre Effekte zu erhalten und zu einem besseren Verständnis der neuronalen Biologie zu gelangen. 1.2.1 Das MFN2-Gen Das MFN2-Gen kodiert das Protein Mitofusin 2 (MFN2) und ist auf Chromosom 1p.36.2 lokalisiert [5]. Der offene Leserahmen umspannt Exon 3 bis 19. Abb. 3 Schematische Darstellung des MFN2-Gens, bestehend aus 19 Exons. Der offene Leserahmen umspannt Exon 3 bis Exon 19. Funktionelle Domänen des Gens: GTPaseRegion, Cc-Region (coiled coil), TM-Region (Transmembranfragment). (modifiziert nach Züchner et al. 2004) Einleitung 8 In Hefen, sowie in der Fruchtfliege Drosophila melanogaster, wird die mitochondriale Fusion durch die nukleär kodierte GTPase fuzzy onions (fzo) kontrolliert [12, 23, 27]. Im Menschen und in Mäusen existieren zwei homologe Proteine des Fzo-Proteins, Mitofusin 1 (MFN1) und MFN2. Sie sind beide essentiell für die embryonale Entwicklung und für die mitochondriale Fusion [12]. MFN2 ist eines der Gene, welches direkt an der Aufrechterhaltung des mitochondrialen Netzwerks beteiligt ist. Mutationen im Ganglioside-Induced-DifferentiationAssociated-Protein-1-Gen (GDAP1 Gen) führen bei Überexpression des Proteins ebenfalls zu eine Störung von Fusionsprozessen. Eine Fragmentierung von Mitochondrien ist die Folge [41, 42]. Autosomal-rezessiv vererbte Mutationen im GDAP1-Gen wurden in Patienten mit CMT4A gefunden. 1.2.2 Aufbau, Lokalisation und Funktion des MFN2-Proteins Das MFN2-Protein ist ein Transmembranprotein, welches in der Außenmembran der Mitochondrien verankert ist. Der Aufbau des Proteins gliedert sich in eine GTPase-Domäne, welche die Energie für mitochondriale Fusionsprozesse sicherstellt, ein Transmembranfragment (TM), welches das Protein in der Mitochondrienwand verankert und zwei angrenzende coiled-coil (Cc) Strukturen (HR1 (heptad repeat regions 1) und HR2 (heptad repeat regions 1)), die wichtig für die Verknüpfung unterschiedlicher Mitochondrien sind. Abb. 4 Schematische Darstellung des MFN2-Proteins in der mitochondrialen Außenmembran (AM). Die GTPase stellt Energie für Fusionsprozesse bereit. HR1 und HR2 Regionen erfüllen ebenfalls wichtige Aufgaben bei der Verknüpfung von Mitochondrien. Einleitung 9 Die Cc-Strukturen bilden antiparallele Dimere, welche Mitochondrien miteinander verbinden, die bereit sind zu fusionieren [29, 34]. Eine intakte Funktion der GTPase ist unverzichtbar für die Funktion des Mitofusins [20, 23, 34]. Zielsetzung der Arbeit 10 2 Zielsetzung der Arbeit Ziel der vorliegenden Arbeit war es, Patienten mit der klinischen Diagnose CMT2 mittels molekulargenetischer Methoden auf Mutationen im MFN2-Gen zu untersuchen. Es sollte ermittelt werden, ob im untersuchten Patientenkollektiv eine Assoziation zwischen Mutationen in diesem Gen und der CMT2Erkrankung existiert. Weiterhin war zu fragen, ob es sich bei einer gegebenen Assoziation sogar um eine der Hauptursachen für die CMT2-Erkrankung handelt. Diese Studie sollte somit einen Beitrag zur Klärung der Krankheitsursache liefern. Die molekulare Diagnostik stellt ein bedeutendes Instrumentarium zur Früherkennung von erblichen Erkrankungen dar. Zu Beginn dieser Studie lagen nur begrenzte Kenntnisse über häufig betroffene Gene der CMT2-Erkrankung vor. Daher sollte diese Studie einen wichtigen Beitrag zur Klärung dieser Fragestellung liefern, und kann mit den Ergebnissen entscheidende Empfehlungen für die molekulare CMT2-Diagnostik geben. Methode und Ergebnisse 11 3 Methode und Ergebnisse 3.1 Mutationsanalyse des MFN2-Gens Für die molekulargenetischen Analysen standen 73 Proben von CMT2Patienten zur Verfügung. Für die Mutationsanalyse wurde Polymerasekettenreaktion (PCR), single strand conformation polymorphism (SSCP) und Sequenzierung genutzt. Die gesunden Kontrollproben wurden mit Hilfe geeigneter Restriktionsenzyme geschnitten, um zu beweisen, dass sie die Mutation der entsprechenden Patientenprobe nicht tragen. Zur SSCP-Analyse wurden die denaturierten Patientenproben auf zwei jeweils in der Zusammensetzung unterschiedliche Polyacrylamidgele (PAA) aufgetragen und mittels Elektrophorese aufgetrennt. Auffällige Proben, welche sich im Laufverhalten von den anderen unterschieden, wurden erneut amplifiziert und sequenziert. Die genaue Aufschlüsselung der Basensequenz durch die Sequenzierung gab Hinweise auf das Vorliegen einer Mutation in der entsprechenden Probe. Um auszuschließen, dass der jeweilige Basenaustausch einen seltenen Polymorphismus darstellt, wurden pro Mutation mindestens 200 gesunde Kontrollchromosomen durch Restriktionsenzyme geschnitten, auf ein Agarosegel aufgetragen und elektrophoretisch getrennt. 3.2 Ergebnisse Die Mutationsanalyse des MFN2-Gens zeigte insgesamt sechs Mutationen, welche in der Literatur zuvor noch nicht beschrieben wurden. Diese Mutationen ließen sich in sechs unterschiedlichen Patienten nachweisen. Jeder der sechs Patienten zeigte jeweils eine Mutation in einem Exon. Insgesamt konnten in fünf unterschiedlichen der 19 Exons Mutationen nachgewiesen werden. Methode und Ergebnisse 12 Abb. 5 Struktur des MFN2-Proteins. Es sind funktionelle Domänen und publizierte Mutationen abgebildet. Die durch vorliegende Studie entdeckten Mutationen sind unterstrichen. Mit HMSN V und HMSN VI assoziierte Mutationen sind mit * und + gekennzeichnet [19]. Eine Mutation in Exon 5 (c.380G>T (G127V)) wurde in der Patientenprobe einer 58 Jahre alten Frau gefunden. Ich entdeckte zwei weitere Mutationen in Exon 11 (c.1128G>A (M376I) und c.1040A>T (E347V)) bei einem 34- bzw. bei einem 32-jährigen Mann. Eine Mutation wurde bei einer 27 Jahre alten Frau in Exon 14 lokalisiert (c.1403G>A (R468H)). Auch in Exon 18 bzw. in Exon 19 konnte bei einer 44 Jahre alten Patientin bzw. bei einem 64 Jahre altem Patienten jeweils eine Mutation aufgespürt werden (c.2113G>A (V705I) und c.2258_2259insT (L753fs)). Der Phänotyp aller Patienten ist in Tabelle 3 und 4 den entsprechenden Mutationen zugeordnet. Methode und Ergebnisse 13 Tab. 3: Mutationsspektrum und klinische Daten der Patienten 1-3 Patient 1 Patient 2 Patient 3 Mutation c.380G>T (G127V) c.1128G>A (M376I) c.1040A>T (E347V) Alter u. Geschlecht des Patienten 58/F 34/F 32/M Erkrankungsalter 48 22 Kindheit Initiale Symptome Muskelschwäche in unterer Extremität Muskelkrämpfe in unterer Extremität Nicht bekannt 53 50 Nicht bekannt NLG (m/s) Nervus medianus (normal : ≥ 50 m/s) Reflexe Pes cavus/varus Normal in Normal in Normal in oberer Extremität, oberer Extremität, oberer Extremität, Achillessehnenreflex Achillessehnenreflex Achillessehnenreflex nicht vorhanden nicht vorhanden nicht vorhanden ja ja Ja Tab. 4: Mutationsspektrum und klinische Daten der Patienten 4-6 Patient 4 Patient 5 Mutation c.1403G>A (R468H) c.2113G>A (V705I) c.2258_2259insT (L753fs) Alter u. Geschlecht des Patienten 27/F 44/F 65/M Erkrankungsalter 26 6 62 Initiale Symptome Parästhesien in unterer Extremität Fußdeformation Gangataxie 46,2 56 Nicht bekannt NLG (m/s) Nervus medianus Patient 6 (normal : ≥ 50 m/s) Reflexe Pes cavus/varus Normal in Erniedrigt in Normal in oberer Extremität, oberer Extremität, oberer Extremität, Achillessehnenreflex Achillessehnenreflex Achillessehnenreflex nicht vorhanden nicht vorhanden nicht vorhanden ja ja Ja Diskussion 14 4 Diskussion In der vorliegenden Studie konnten bei einem CMT2-Kollektiv von 73 Patienten in sechs Fällen Mutationen nachgewiesen werden. Keine der Mutationen wurde zuvor in der Literatur beschrieben und bis auf eine Mutation ließ sich keine der weiteren Mutationen in anonymen Kontrollen nachweisen [32, 36, 63-65]. Somit beträgt die Mutationsrate dieses Kollektivs 8 %. Die Rate ist mit den Detektionsraten von 10-20 % anderer Arbeitsgruppen vergleichbar. Meine Daten unterstützen die These, dass Mutationen im MFN2-Gen eine große Rolle bei der Pathogenese von Charcot-Marie-Tooth Neuropathien vom Typ 2 einnehmen. Obwohl Patienten mit HMSN V und HMSN VI ebenfalls Mutationen im MFN2Gen aufweisen, ließen sich in Patienten dieser Studie keine zusätzlichen Symptome wie Pyramidenbahnzeichen und Optikusatrophie nachweisen [64]. Die Patientensymptome in der vorliegenden Studie können als mäßig ausgeprägt beschrieben werden und die Progression verläuft relativ langsam. Bei zwei Drittel der Patienten manifestierte sich die Erkrankung erst relativ spät (>10 Jahre alt, late onset). Im Vordergrund stehen Fußdeformationen, Muskelschwäche und Sensitivitätsverlust in der unteren Extremität. Nur ein Patient zeigte eine Abschwächung der Reflexe der oberen Extremität (c.2113G>A (V705I)). Keiner der Patienten ist bis jetzt rollstuhlabhängig. Die mNLG weist in allen Fällen auf eine axonale Polyneuropathie hin. In der Literatur wird zunehmend der Zusammenhang von MFN2-Mutationen und peripheren Polyneuropathien hergestellt [65]. Die Physiologie der mitochondrialen Netzwerke im peripherem Nerv, die Rolle des Proteins MFN2 und letztendlich die Auswirkungen von Mutationen im MFN2-Gen sind allerdings nur teilweise bekannt. Mitochondrien sind aktive Organellen, welche ständigen Teilungs- und Fusionsprozessen unterworfen sind [43]. Sie bilden in Zellen netzwerkartige Strukturen aus, um die Energieversorgung auch über große Distanzen aufrecht zu erhalten. In der Fruchtfliege Drosophila melanogaster, wie auch in Hefen, wird die mitochondriale Fusion von der GTPase fzo kontrolliert [12, 23, 27]. In Menschen und Mäusen kontrollieren, homolog zu fzo, MFN1 und MFN2 die Fusionsprozesse der Mitochondrien. Es wurde nachgewiesen, dass ein Fehlen von MFN1 Diskussion 15 oder MFN2 zu fehlerhafter Embryonalentwicklung und vollständiger Fragmentierung von mitochondrialen Netzwerken führt [12]. Eine Fusionsaktivität konnte nicht mehr beobachtet werden. Die mitochondriale Morphologie ist ebenso entscheidend für das Zellwachstum, das mitochondriale Membranpotential und die Zellatmung. MFN2 ist in der äußeren Membran der Mitochondrien verankert. Der NTerminus sowie der C-Terminus ragen in das Zytosol hinein. Der N-Terminus besteht aus einer GTPase Domäne und wird über eine Cc-Domäne mit dem TM-Fragment, welches das Protein in der Membran befestigt, verbunden. Dem TM-Fragment ist auf der C-terminalen Seite eine zweite Cc-Region angeschlossen. Eine funktionierende GTPase-Domäne ist unverzichtbar für die Funktion des Proteins [20, 23, 47]. Ebenso wichtig ist die Funktion der Cc-Regionen. Über diese werden Verbindungen mit benachbarten Mitochondrien hergestellt, um Fusionsprozesse durchführen zu können [28]. Ein weiteres Gen ist ebenfalls bei Fusionsprozessen der Mitochondrien beteiligt. Optic-Atrophy-1- (OPA1)- Mutationen sind eine der häufigsten Ursachen für autosomal-dominant vererbte Optikusatrophien [1]. Kürzlich konnte auch eine Beteiligung von MFN2-Mutationen an der Entstehung von Optikusatrophien nachgewiesen werden [64]. GDAP1-Mutationen führen zu einer Überexpression des Proteins und dadurch zu Störungen mitochondrialer Fusionsprozesse. Autosomal-rezessive Mutationen lassen sich bei CMT4A-Patienten finden [41, 42]. Zum Zeitpunkt der Veröffentlichung sind 22 verschiedene Mutationen im MFN2Gen bekannt, welche eine CMT2 oder eine HMSN V und HMSN VI auslösen [32, 36, 63-65]. Bis heute ist noch nicht geklärt, wie es zu der recht unterschiedlichen Genotyp-Phänotyp-Relation kommt [65]. Weitere Untersuchungen zur Dynamik von Mitochondrien werden nötig sein, um zu verstehen, warum Mutationen in unterschiedlichen Genen zu gleichen oder unterschiedlichen Phänotypen führen. Obwohl andere Arbeitsgruppen Mutationen in besonderen hot spot Regionen des MFN2-Gens beschreiben (aa94, aa236-251, aa273-284, aa357-364), wurde in diesem Kollektiv keine der bisher entdecken Mutationen wieder gefunden. Dies könnte darauf hindeuten, dass die unterschiedlichen untersuchten Patien- Diskussion 16 tenkollektive verschiedener Arbeitsgruppen ethnische Unterschiede aufweisen. Möglich wäre auch, dass zu wenig Patienten für diese Studie zur Verfügung standen und somit auch weniger Mutationen gefunden werden konnten. Fünf von sechs Mutationen in unserem Kollektiv sind missense-Mutationen. Eine Mutation befindet sich direkt in der für die GTPase kodierenden Region (G127V). Zwei Mutationen sind zwischen der GTPase-Region (E347V) und der ersten Cc-Region (M376I) lokalisiert. Eine Mutation befindet sich ebenfalls nahe der ersten Cc-Region (R468H). Zwei weitere Mutationen betreffen den Bereich oberhalb der TM-Region (V705I) und der zweiten Cc-Region (L753fs) (siehe Abb.5). Die Mutation E347V liegt in einer hoch konservierten Region des Gens, welche möglicherweise unterstützende Funktionen beim Fusionieren von Mitochondrien einnimmt und somit essentiell für die Funktion von MFN2 zu sein scheint [28]. In Deletionskonstrukten für MFN2 wurde gezeigt, dass GTPase-abhängige Interaktionen zwischen dem N-Terminus und der sich am C-Terminus des Proteins befindenden Cc-Region stattfinden. Diese Interaktionen dienen ebenfalls der Fusion von Mitochondrien. Es wird auch vermutet, dass der C-Terminus wichtige Regionen enthält, welche das Targeting zwischen Protein und Mitochondrienmembran sicherstellen [28]. Die Frameshiftmutation L753fs befindet sich am Ende der zweiten Cc-Region am C-terminalem Ende des Proteins. Das Protein unterscheidet sich nur in vier Aminosäuren und einer Substitution von 5 weiteren Aminosäuren vom ursprünglichem Protein. Weitere Studien von Promotor-Regionen werden nötig sein, um zu klären, ob diese Region bei der Ausbildung von CMT2 beteiligt ist. Zu Beginn dieser Studie waren nur wenige Daten über CMT2-Erkrankungen und Mutationen im MFN2-Gen bekannt. Diese Studie konnte eine Assoziation zwischen MFN2-Mutationen und CMT2-Neuropathien nachweisen. Somit liefert sie neben anderen Veröffentlichungen einen wichtigen Beitrag zur Erforschung von hereditären Neuropathien und deren Ursachen. Die Mutationsrate von 8 % in diesem Patientenkollektiv weist darauf hin, dass MFN2-Mutationen zu den häufigsten Ursachen der CMT2 zählen. Eine molekulargenetische Diagnostik des MFN2-Gens sollte deshalb in die Laborroutine zur Testung aufgenommen werden. Literaturverzeichnis 17 5 Literaturverzeichnis [1] Alexander, C., Votruba, M., Pesch, U.E., Thiselton, D.L., Mayer, S., Moore, A., Rodriguez, M., Kellner, U., Leo-Kottler, B., Auburger, G., Bhattacharya, S.S. and Wissinger, B. (2000). OPA1, encoding a dynaminrelated GTPase, is mutated in autosomal dominant optic atrophy linked to chromosome 3q28. Nat Genet 26, 211-215. [2] Antonellis, A., Ellsworth, R.E., Sambuughin, N., Puls, I., Abel, A., LeeLin, S.Q., Jordanova, A., Kremensky, I., Christodoulou, K., Middleton, L.T., Sivakumar, K., Ionasescu, V., Funalot, B., Vance, J.M., Goldfarb, L.G., Fischbeck, K.H. and Green, E.D. (2003). Glycyl tRNA synthetase mutations in Charcot-Marie-Tooth disease type 2D and distal spinal muscular atrophy type V. Am J Hum Genet 72, 1293-1299. [3] Bakeeva, L.E., Chentsov Yu, S. and Skulachev, V.P. (1978). Mitochondrial framework (reticulum mitochondriale) in rat diaphragm muscle. Biochim Biophys Acta 501, 349-369. [4] Barhoumi, C., Amouri, R., Ben Hamida, C., Ben Hamida, M., Machghoul, S., Gueddiche, M. and Hentati, F. (2001). Linkage of a new locus for autosomal recessive axonal form of Charcot-Marie-Tooth disease to chromosome 8q21.3. Neuromuscul Disord 11, 27-34. [5] Ben Othmane, K., Middleton, L.T., Loprest, L.J., Wilkinson, K.M., Lennon, F., Rozear, M.P., Stajich, J.M., Gaskell, P.C., Roses, A.D., PericakVance, M.A. and et al. (1993). Localization of a gene (CMT2A) for autosomal dominant Charcot-Marie-Tooth disease type 2 to chromosome 1p and evidence of genetic heterogeneity. Genomics 17, 370-375. [6] Berghoff, C., Berghoff, M., Leal, A., Morera, B., Barrantes, R., Reis, A., Neundorfer, B., Rautenstrauss, B., Del Valle, G. and Heuss, D. (2004). Clinical and electrophysiological characteristics of autosomal recessive axonal Charcot-Marie-Tooth disease (ARCMT2B) that maps to chromosome 19q13.3. Neuromuscul Disord 14, 301-306. [7] Boerkoel, C.F., Takashima, H., Garcia, C.A., Olney, R.K., Johnson, J., Berry, K., Russo, P., Kennedy, S., Teebi, A.S., Scavina, M., Williams, L.L., Mancias, P., Butler, I.J., Krajewski, K., Shy, M. and Lupski, J.R. (2002). Charcot-Marie-Tooth disease and related neuropathies: mutation distribution and genotype-phenotype correlation. Ann Neurol 51, 190201. [8] Chalmers, R.M., Bird, A.C. and Harding, A.E. (1996). Autosomal dominant optic atrophy with asymptomatic peripheral neuropathy. J Neurol Neurosurg Psychiatry 60, 195-196. [9] Charcot-Marie-Tooth Neuropathy Type 1. (Zugriff vom 01.05.2007). http://www.ncbi.nlm.nih.gov/books/bv.fcgi?indexed=google&rid=gene.cha pter.cmt1 Literaturverzeichnis 18 [10] Charcot-Marie-Tooth Neuropathy Type 2. (Zugriff vom 01.05.2007). http://www.ncbi.nlm.nih.gov/books/bv.fcgi?indexed=google&rid=gene.cha pter.cmt2 [11] Chen, H. and Chan, D.C. (2006). Critical dependence of neurons on mitochondrial dynamics. Curr Opin Cell Biol 18, 453-459. [12] Chen, H., Detmer, S.A., Ewald, A.J., Griffin, E.E., Fraser, S.E. and Chan, D.C. (2003). Mitofusins Mfn1 and Mfn2 coordinately regulate mitochondrial fusion and are essential for embryonic development. J Cell Biol 160, 189-200. [13] Cuesta, A., Pedrola, L., Sevilla, T., Garcia-Planells, J., Chumillas, M.J., Mayordomo, F., LeGuern, E., Marin, I., Vilchez, J.J. and Palau, F. (2002). The gene encoding ganglioside-induced differentiation-associated protein 1 is mutated in axonal Charcot-Marie-Tooth type 4A disease. Nat Genet 30, 22-25. [14] Davis, C.J., Bradley, W.G. and Madrid, R. (1978). The peroneal muscular atrophy syndrome: clinical, genetic, electrophysiological and nerve biopsy studies. I. Clinical, genetic and electrophysiological findings and classification. J Genet Hum 26, 311-349. [15] De Jonghe, P., Timmerman, V., Ceuterick, C., Nelis, E., De Vriendt, E., Lofgren, A., Vercruyssen, A., Verellen, C., Van Maldergem, L., Martin, J.J. and Van Broeckhoven, C. (1999). The Thr124Met mutation in the peripheral myelin protein zero (MPZ) gene is associated with a clinically distinct Charcot-Marie-Tooth phenotype. Brain 122 (Pt 2), 281-290. [16] De Sandre-Giovannoli, A., Chaouch, M., Kozlov, S., Vallat, J.M., Tazir, M., Kassouri, N., Szepetowski, P., Hammadouche, T., Vandenberghe, A., Stewart, C.L., Grid, D. and Levy, N. (2002). Homozygous defects in LMNA, encoding lamin A/C nuclear-envelope proteins, cause autosomal recessive axonal neuropathy in human (Charcot-Marie-Tooth disorder type 2) and mouse. Am J Hum Genet 70, 726-736. [17] Dimauro, S. and Davidzon, G. (2005). Mitochondrial DNA and disease. Ann Med 37, 222-232. [18] Dyck, P.J. and Lambert, E.H. (1968). Lower motor and primary sensory neuron diseases with peroneal muscular atrophy. I. Neurologic, genetic, and electrophysiologic findings in hereditary polyneuropathies. Arch Neurol 18, 603-618. [19] Engelfried, K., Vorgerd, M., Hagedorn, M., Haas, G., Gilles, J., Epplen, J.T. and Meins, M. (2006). Charcot-Marie-Tooth neuropathy type 2A: novel mutations in the mitofusin 2 gene (MFN2). BMC Med Genet 7, 53. [20] Eura, Y., Ishihara, N., Yokota, S. and Mihara, K. (2003). Two mitofusin proteins, mammalian homologues of FZO, with distinct functions are both required for mitochondrial fusion. J Biochem (Tokyo) 134, 333-344. Literaturverzeichnis 19 [21] Evgrafov, O.V., Mersiyanova, I., Irobi, J., Van Den Bosch, L., Dierick, I., Leung, C.L., Schagina, O., Verpoorten, N., Van Impe, K., Fedotov, V., Dadali, E., Auer-Grumbach, M., Windpassinger, C., Wagner, K., Mitrovic, Z., Hilton-Jones, D., Talbot, K., Martin, J.J., Vasserman, N., Tverskaya, S., Polyakov, A., Liem, R.K., Gettemans, J., Robberecht, W., De Jonghe, P. and Timmerman, V. (2004). Mutant small heat-shock protein 27 causes axonal Charcot-Marie-Tooth disease and distal hereditary motor neuropathy. Nat Genet 36, 602-606. [22] Ferreirinha, F., Quattrini, A., Pirozzi, M., Valsecchi, V., Dina, G., Broccoli, V., Auricchio, A., Piemonte, F., Tozzi, G., Gaeta, L., Casari, G., Ballabio, A. and Rugarli, E.I. (2004). Axonal degeneration in paraplegin-deficient mice is associated with abnormal mitochondria and impairment of axonal transport. J Clin Invest 113, 231-242. [23] Hales, K.G. and Fuller, M.T. (1997). Developmentally regulated mitochondrial fusion mediated by a conserved, novel, predicted GTPase. Cell 90, 121-129. [24] Harding, A.E. and Thomas, P.K. (1980). The clinical features of hereditary motor and sensory neuropathy types I and II. Brain 103, 259-280. [25] Harding, A.E. and Thomas, P.K. (1984). Peroneal muscular atrophy with pyramidal features. J Neurol Neurosurg Psychiatry 47, 168-172. [26] Hayasaka, K., Himoro, M., Sato, W., Takada, G., Uyemura, K., Shimizu, N., Bird, T.D., Conneally, P.M. and Chance, P.F. (1993). Charcot-MarieTooth neuropathy type 1B is associated with mutations of the myelin P0 gene. Nat Genet 5, 31-34. [27] Hermann, G.J. and Shaw, J.M. (1998). Mitochondrial dynamics in yeast. Annu Rev Cell Dev Biol 14, 265-303. [28] Honda, S., Aihara, T., Hontani, M., Okubo, K. and Hirose, S. (2005). Mutational analysis of action of mitochondrial fusion factor mitofusin-2. J Cell Sci 118, 3153-3161. [29] Honda, S. and Hirose, S. (2003). Stage-specific enhanced expression of mitochondrial fusion and fission factors during spermatogenesis in rat testis. Biochem Biophys Res Commun 311, 424-432. [30] Houlden, H. and Reilly, M.M. (2006). Molecular genetics of autosomaldominant demyelinating Charcot-Marie-Tooth disease. Neuromolecular Med 8, 43-62. [31] Inherited Peripheral Neuropathy Mutation Database. (Zugriff vom 01.05.2007). http://www.molgen.ua.ac.be/CMTMutations [32] Kijima, K., Numakura, C., Izumino, H., Umetsu, K., Nezu, A., Shiiki, T., Ogawa, M., Ishizaki, Y., Kitamura, T., Shozawa, Y. and Hayasaka, K. Literaturverzeichnis 20 (2005). Mitochondrial GTPase mitofusin 2 mutation in Charcot-MarieTooth neuropathy type 2A. Hum Genet 116, 23-27. [33] Klein, C.J., Cunningham, J.M., Atkinson, E.J., Schaid, D.J., Hebbring, S.J., Anderson, S.A., Klein, D.M., Dyck, P.J., Litchy, W.J., Thibodeau, S.N. and Dyck, P.J. (2003). The gene for HMSN2C maps to 12q23-24: a region of neuromuscular disorders. Neurology 60, 1151-1156. [34] Koshiba, T., Detmer, S.A., Kaiser, J.T., Chen, H., McCaffery, J.M. and Chan, D.C. (2004). Structural basis of mitochondrial tethering by mitofusin complexes. Science 305, 858-862. [35] Kuhlenbäumer, G., Young, P., Hunermund, G., Ringelstein, B. and Stogbauer, F. (2002). Clinical features and molecular genetics of hereditary peripheral neuropathies. J Neurol 249, 1629-1650. [36] Lawson, V.H., Graham, B.V. and Flanigan, K.M. (2005). Clinical and electrophysiologic features of CMT2A with mutations in the mitofusin 2 gene. Neurology 65, 197-204. [37] Lupski, J.R., de Oca-Luna, R.M., Slaugenhaupt, S., Pentao, L., Guzzetta, V., Trask, B.J., Saucedo-Cardenas, O., Barker, D.F., Killian, J.M., Garcia, C.A., Chakravarti, A. and Patel, P.I. (1991). DNA duplication associated with Charcot-Marie-Tooth disease type 1A. Cell 66, 219-232. [38] Marrosu, M.G., Vaccargiu, S., Marrosu, G., Vannelli, A., Cianchetti, C. and Muntoni, F. (1998). Charcot-Marie-Tooth disease type 2 associated with mutation of the myelin protein zero gene. Neurology 50, 1397-1401. [39] Mersiyanova, I.V., Perepelov, A.V., Polyakov, A.V., Sitnikov, V.F., Dadali, E.L., Oparin, R.B., Petrin, A.N. and Evgrafov, O.V. (2000). A new variant of Charcot-Marie-Tooth disease type 2 is probably the result of a mutation in the neurofilament-light gene. Am J Hum Genet 67, 37-46. [40] Nelis, E., Berciano, J., Verpoorten, N., Coen, K., Dierick, I., Van Gerwen, V., Combarros, O., De Jonghe, P. and Timmerman, V. (2004). Autosomal dominant axonal Charcot-Marie-Tooth disease type 2 (CMT2G) maps to chromosome 12q12-q13.3. J Med Genet 41, 193-197. [41] Nelis, E., Erdem, S., Van Den Bergh, P.Y., Belpaire-Dethiou, M.C., Ceuterick, C., Van Gerwen, V., Cuesta, A., Pedrola, L., Palau, F., GabreelsFesten, A.A., Verellen, C., Tan, E., Demirci, M., Van Broeckhoven, C., De Jonghe, P., Topaloglu, H. and Timmerman, V. (2002). Mutations in GDAP1: autosomal recessive CMT with demyelination and axonopathy. Neurology 59, 1865-1872. [42] Niemann, A., Ruegg, M., La Padula, V., Schenone, A. and Suter, U. (2005). Ganglioside-induced differentiation associated protein 1 is a regulator of the mitochondrial network: new implications for CharcotMarie-Tooth disease. J Cell Biol 170, 1067-1078. Literaturverzeichnis 21 [43] Nunnari, J., Marshall, W.F., Straight, A., Murray, A., Sedat, J.W. and Walter, P. (1997). Mitochondrial transmission during mating in Saccharomyces cerevisiae is determined by mitochondrial fusion and fission and the intramitochondrial segregation of mitochondrial DNA. Mol Biol Cell 8, 1233-1242. [44] Palay, S.L. (1956). Synapses in the central nervous system. J Biophys Biochem Cytol 2, 193-202. [45] Raeymaekers, P., Timmerman, V., Nelis, E., De Jonghe, P., Hoogendijk, J.E., Baas, F., Barker, D.F., Martin, J.J., De Visser, M., Bolhuis, P.A. and et al. (1991). Duplication in chromosome 17p11.2 in Charcot-Marie-Tooth neuropathy type 1a (CMT 1a). The HMSN Collaborative Research Group. Neuromuscul Disord 1, 93-97. [46] Reichert, A.S. and Neupert, W. (2004). Mitochondriomics or what makes us breathe. Trends Genet 20, 555-562. [47] Santel, A. and Fuller, M.T. (2001). Control of mitochondrial morphology by a human mitofusin. J Cell Sci 114, 867-874. [48] Shaw, J.M. and Nunnari, J. (2002). Mitochondrial dynamics and division in budding yeast. Trends Cell Biol 12, 178-184. [49] Skre, H. (1974). Genetic and clinical aspects of Charcot-Marie-Tooth's disease. Clin Genet 6, 98-118. [50] Skulachev, V.P. (2001). Mitochondrial filaments and clusters as intracellular power-transmitting cables. Trends Biochem Sci 26, 23-29. [51] Street, V.A., Bennett, C.L., Goldy, J.D., Shirk, A.J., Kleopa, K.A., Tempel, B.L., Lipe, H.P., Scherer, S.S., Bird, T.D. and Chance, P.F. (2003). Mutation of a putative protein degradation gene LITAF/SIMPLE in CharcotMarie-Tooth disease 1C. Neurology 60, 22-26. [52] Suter, U. and Scherer, S.S. (2003). Disease mechanisms in inherited neuropathies. Nat Rev Neurosci 4, 714-726. [53] Tang, B.S., Luo, W., Xia, K., Xiao, J.F., Jiang, H., Shen, L., Tang, J.G., Zhao, G.H., Cai, F., Pan, Q., Dai, H.P., Yang, Q.D., Xia, J.H. and Evgrafov, O.V. (2004). A new locus for autosomal dominant Charcot-MarieTooth disease type 2 (CMT2L) maps to chromosome 12q24. Hum Genet 114, 527-533. [54] Taylor, R.W. and Turnbull, D.M. (2005). Mitochondrial DNA mutations in human disease. Nat Rev Genet 6, 389-402. [55] Thomas, P.K., King, R.H., Small, J.R. and Robertson, A.M. (1996). The pathology of charcot-marie-tooth disease and related disorders. Neuropathol Appl Neurobiol 22, 269-284. Literaturverzeichnis 22 [56] Timmerman, V., De Jonghe, P., Spoelders, P., Simokovic, S., Lofgren, A., Nelis, E., Vance, J., Martin, J.J. and Van Broeckhoven, C. (1996). Linkage and mutation analysis of Charcot-Marie-Tooth neuropathy type 2 families with chromosomes 1p35-p36 and Xq13. Neurology 46, 13111318. [57] Valentijn, L.J., Baas, F., Wolterman, R.A., Hoogendijk, J.E., van den Bosch, N.H., Zorn, I., Gabreels-Festen, A.W., de Visser, M. and Bolhuis, P.A. (1992). Identical point mutations of PMP-22 in Trembler-J mouse and Charcot-Marie-Tooth disease type 1A. Nat Genet 2, 288-291. [58] Valentijn, L.J., Bolhuis, P.A., Zorn, I., Hoogendijk, J.E., van den Bosch, N., Hensels, G.W., Stanton, V.P., Jr., Housman, D.E., Fischbeck, K.H., Ross, D.A. and et al. (1992). The peripheral myelin gene PMP-22/GAS-3 is duplicated in Charcot-Marie-Tooth disease type 1A. Nat Genet 1, 166170. [59] Vance, J.M. (2000). The many faces of Charcot-Marie-Tooth disease. Arch Neurol 57, 638-640. [60] Verhoeven, K., De Jonghe, P., Coen, K., Verpoorten, N., AuerGrumbach, M., Kwon, J.M., FitzPatrick, D., Schmedding, E., De Vriendt, E., Jacobs, A., Van Gerwen, V., Wagner, K., Hartung, H.P. and Timmerman, V. (2003). Mutations in the small GTP-ase late endosomal protein RAB7 cause Charcot-Marie-Tooth type 2B neuropathy. Am J Hum Genet 72, 722-727. [61] Warner, L.E., Mancias, P., Butler, I.J., McDonald, C.M., Keppen, L., Koob, K.G. and Lupski, J.R. (1998). Mutations in the early growth response 2 (EGR2) gene are associated with hereditary myelinopathies. Nat Genet 18, 382-384. [62] Zhao, C., Takita, J., Tanaka, Y., Setou, M., Nakagawa, T., Takeda, S., Yang, H.W., Terada, S., Nakata, T., Takei, Y., Saito, M., Tsuji, S., Hayashi, Y. and Hirokawa, N. (2001). Charcot-Marie-Tooth disease type 2A caused by mutation in a microtubule motor KIF1Bbeta. Cell 105, 587597. [63] Zhu, D., Kennerson, M.L., Walizada, G., Züchner, S., Vance, J.M. and Nicholson, G.A. (2005). Charcot-Marie-Tooth with pyramidal signs is genetically heterogeneous: families with and without MFN2 mutations. Neurology 65, 496-497. [64] Züchner, S., De Jonghe, P., Jordanova, A., Claeys, K.G., Guergueltcheva, V., Cherninkova, S., Hamilton, S.R., Van Stavern, G., Krajewski, K.M., Stajich, J., Tournev, I., Verhoeven, K., Langerhorst, C.T., de Visser, M., Baas, F., Bird, T., Timmerman, V., Shy, M. and Vance, J.M. (2006). Axonal neuropathy with optic atrophy is caused by mutations in mitofusin 2. Ann Neurol 59, 276-281. Literaturverzeichnis [65] 23 Züchner, S., Mersiyanova, I.V., Muglia, M., Bissar-Tadmouri, N., Rochelle, J., Dadali, E.L., Zappia, M., Nelis, E., Patitucci, A., Senderek, J., Parman, Y., Evgrafov, O., Jonghe, P.D., Takahashi, Y., Tsuji, S., Pericak-Vance, M.A., Quattrone, A., Battaloglu, E., Polyakov, A.V., Timmerman, V., Schröder, J.M. and Vance, J.M. (2004). Mutations in the mitochondrial GTPase mitofusin 2 cause Charcot-Marie-Tooth neuropathy type 2A. Nat Genet 36, 449-451. Danksagung 6 Danksagung Mein Dank gilt vielen Leuten, die mich auf verschiedenste Art und Weise unterstütz haben: Herrn PD Dr. med. Moritz Meins und Herrn Prof. Dr. med. Jörg T. Epplen für eine hervorragende Betreuung, den Mitarbeitern der Abteilung für Humangenetik Bochum für meine erlernten technischen Fähigkeiten und dafür, dass sie immer ein offenes Ohr für mich hatten, Herrn Prof. Dr. med. Matthias Vorgerd, Stefan Woeste, Alexandra Engelfried. Vielen Dank! Lebenslauf Lebenslauf PERSÖNLICHE DATEN: Vorname: Kathrin Nachname: Engelfried Geburtstag: 27. Juli 1978 Geburtsort: Esslingen (am Neckar) AUSBILDUNG/ STUDIUM/ FORTBILDUNG: 1989 – 1998 Friedrich-Harkort-Gymnasium Herdecke, Abitur 1999 Ausbildung zur Rettungssanitäterin, DRK Landesschule Münster 1999 – 2001 Ausbildung zur Rettungsassistentin, WestfalenSchulen Dortmund; Feuerwehr Hattingen 2001 – 2003 Ruhr-Universität Bochum, Vorklinik September 2003 Physikum seit 2003 Ruhr-Universität Bochum, klinischer Abschnitt Juni 2004 Beginn einer experimentellen, prospektiven Doktorarbeit in der Abteilung für Humangenetik, Ruhr-Universität Bochum Oktober 2004 – Februar 2005 Wahlseminare Schmerztherapie, Wahlseminar Akupunktur, Wahlseminar EKG-Analyse, Wahlseminar Anästhesie, Wahlseminar Naturheilkunde an der Ruhr-Universität Bochum März 2006 Wahlseminar Echokardiographie und Herzgeräusche, Gernsbach August 2006 Wahlseminar Asthma und Allergie, Davos (Schweiz) Lebenslauf August 2006 – August 2007 Praktisches Jahr im Allgemeinen Krankenhaus in Hagen, Wahlfach: Anästhesie voraussichtlich Mai 2008 Zweiter Abschnitt der Ärztlichen Prüfung FAMULATUREN: Februar 2004 – März 2004 Marienhospital Witten, Famulatur in der Kinderklinik März 2004 – April 2004 Berufsgenossenschaftliche Kliniken Bergmannsheil, Famulatur in der Abteilung für Anästhesie, Intensivmedizin und Schmerztherapie August 2004 – September 2004 Ruhr-Universität Bochum, Famulatur in der Abteilung für Humangenetik September 2004 Dr. med Holz & Dr. med Bocksch, Famulatur in einer Praxis für Innere Medizin (Schwerpunkt Gastroenterologie) Juli 2005 – September 2005 University of Southern California, Los Angeles, USA, Famulatur in der Abteilung für Pulmonologie und Intensivmedizin des Los Angeles County Hospital Oktober 2005 Uniklinik St. Josef Hospital Bochum, Famulatur in der Abteilung für Neurologie April 2006 Marienhospital Witten, Famulatur in der Abteilung für Anästhesie und Intensivmedizin Juni 2006 University Hospital Galway, Irland, Famulatur in der interdisziplinären Notaufnahme (Accident & Emergency) BMC Medical Genetics BioMed Central Open Access Research article Charcot-Marie-Tooth neuropathy type 2A: novel mutations in the mitofusin 2 gene (MFN2) Kathrin Engelfried1, Matthias Vorgerd2, Michaela Hagedorn1, Gerhard Haas3, Jürgen Gilles4, Jörg T Epplen1 and Moritz Meins*1 Address: 1Department of Human Genetics, Ruhr-University Bochum, Germany, 2Department of Neurology, Neuromuscular Center Ruhrgebiet, Ruhr-University Bochum, Germany, 3Neurology, Evangelische Stiftung Tannenhof, Remscheid, Germany and 4Neurology, St.-Marien-Hospital, Lünen, Germany Email: Kathrin Engelfried - [email protected]; Matthias Vorgerd - [email protected]; Michaela Hagedorn - [email protected]; Gerhard Haas - [email protected]; Jürgen Gilles - [email protected]; Jörg T Epplen - [email protected]; Moritz Meins* - [email protected] * Corresponding author Published: 08 June 2006 BMC Medical Genetics 2006, 7:53 doi:10.1186/1471-2350-7-53 Received: 03 April 2006 Accepted: 08 June 2006 This article is available from: http://www.biomedcentral.com/1471-2350/7/53 © 2006 Engelfried et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Charcot-Marie-Tooth neuropathies are a group of genetically heterogeneous diseases of the peripheral nervous system. Mutations in the MFN2 gene have been reported as the primary cause of Charcot-Marie-Tooth disease type 2A. Methods: Patients with the clinical diagnosis of Charcot-Marie-Tooth type 2 were screened using single strand conformation polymorphism (SSCP). All DNA samples showing band shifts in the SSCP analysis were amplified from genomic DNA and cycle sequenced. Results: We analyzed a total of 73 unrelated patients with a clinical diagnosis of CMT 2. Overall, novel mutations were detected in 6 patients. c.380G>T (G127V), c.1128G>A (M376I), c.1040A>T (E347V), c.1403G>A (R468H), c.2113G>A (V705I), and c.2258_2259insT (L753fs). Conclusion: We confirmed a significant role of mutations in MFN2 in the pathogenesis of Charcot-Marie-Tooth disease type 2. Background Charcot-Marie-Tooth neuropathies (CMT), also named as hereditary motor and sensory neuropathies (HMSN) are a group of genetically heterogeneous diseases of the peripheral nervous system. CMT has been classified into two major subgroups. A severe reduction of nerve conduction velocities (NCV) with NCV < 38 m/s is found in the demyelinating CMT type 1. The axonal type (CMT type 2) is characterized by preferential degeneration of the axon showing amplitude reductions in nerve conduction studies but only mildly reduced NCV. Both CMT1 and CMT2 have been recognized to be genetically heterogeneous. Several genetic loci have been defined for both clinical types. CMT2A was located to chromosome 1p35–p36 [13]. Although a mutation in KIF1B was published in a large CMT2A family, no further mutations were detected in other families with CMT2A [4,5]. Züchner et al. identified the MFN2 gene by means of linkage studies and reported mutations in MFN2 in seven large families with linkage to the CMT2A locus [5]. Recently, other groups confirmed the MFN2 gene as the primary cause of CMT2A [6-8]. We screened 73 unrelated patients with the clinical diagnosis Page 1 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 of CMT2 and identified six new disease-causing mutations. Methods Subjects We analyzed samples of 73 unrelated patients sent to our diagnostic laboratory with the request of genetic analysis for Charcot-Marie-Tooth disease. Linkage analysis was not possible in these individuals. Inclusion criteria for the MFN2 analysis were a clinical classification of CMT2, nerve conduction velocity (NCV) > 38 m/s, or histological findings of axonal degeneration. EDTA blood samples were taken from patients after informed consent. DNA was extracted from blood leukocytes by standard methods. All control samples used to check the distribution of sequence alterations mentioned in the results sections were taken from an anonymous collective of ethnically matched samples. Mutation analysis of MFN2 gene For mutation analysis in MFN2, primers were designed to amplify all exons including flanking intronic regions. Primer sequences are available on request. Exon 7 and 8, and exon 10 and 11, respectively, were each amplified in one amplicon including the intermediate intron. PCRs were performed in 96-well microtiter plates (Thermowell Costar Corning, NY) using a thermocycler (Biometra, Goettingen, Germany). Each well contained 50 ng DNA in 10 µl reaction volume, GC buffer (Genecraft, Münster, Germany), 10 pMol of forward and reverse primer, 1 U Taq Polymerase (Genecraft, Münster, Germany), 2 mMol of each dNTP, and a MgCl2 concentration of 1 mM. For SSCP analysis, 0.06 µl of [α32 P] dCTP (10 mCi/ml) was included in the PCR. PCR conditions included initial denaturation (2 min at 94°C), two initial cycles at 94°C (15 s) and 6°C and 3°C above the main annealing temperature (30 s) followed by 30 s at 72°C, and 28–32 cycles of 94°C (15 s), annealing temperature (30 s) and final elongation step at 72°C (30 s). Annealing temperature was 62°C except for exons 7/8, 10/11, 15, 16, 17, and 8 (58°C). PCR products were digested with suitable restriction enzymes depending on the fragment size to optimize the mutation detection rate by SSCP analysis. In the SSCP analysis the denatured PCR products were separated by polyacrylamide (PAA) gel electrophoresis using two different conditions: 30% PAA (acrylamide/bisacrylamide: 19/1) gel, 1xTBE, and either 10% glycerol or 5% glycerol/ 1 M urea. Electrophoresis was carried out at 55 W for 3–4 h at 4°C. Gels were evaluated by autoradiography or exposure to a phosphoimager screen, using the corresponding software. Exon 13 was screened using SSCP and DHPLC. DNA samples showing band shifts in the SSCP analysis were amplified from genomic DNA and cycle sequenced by standard protocols using the Megabace 1000 (Amersham Bioscience, Freiburg, Germany). If pos- http://www.biomedcentral.com/1471-2350/7/53 sible, restriction analysis with a suitable restriction enzyme was applied to confirm the mutation and to analyse control samples. Enzymes were ordered from New England Biolabs if not indicated otherwise. Results We analyzed a total of 73 unrelated patients with a clinical diagnosis of CMT 2. Overall, novel mutations were detected in 6 patients. The clinical features and the neurographical data of these patients are summarized (tables 1 and 2). Nerve biopsy has not been performed in any of these 6 patients. The heterozygous point mutation c.380 G>T in exon 5 of MFN2 (fig. 1a) was detected in a 58 year old female patient (patient 1), predicting the exchange of Glycine to Valine at position 127 of the MFN2 protein (G127V). The mutation leads to a loss of a recognition site for the restriction enzyme Msc I, which was used to exclude this mutation in 97 control persons (194 control chromosomes). Clinically the patient shows a predominant axonal neuropathy with normal motor nerve conduction velocity (mNCV) in electrophysiological studies of the median nerve. The family history is compatible with autosomaldominant inheritance, but other family members were not available for genetic analysis. Patient 2, a 34 year old male, is heterozygous for the point mutation c.1128G>A in exon 11, predicting the exchange of Methionine to Isoleucine at position 376 (M376I) (fig. 1b). This mutation is detectable by a loss of a NlaIII restriction site, and was excluded by restriction analysis in 190 control chromosomes. The patient has distal sensory loss in his legs, absent Achilles' tendon reflexes, pes cavus and severely reduced amplitudes of the compound motor nerve action potentials of the peroneal and tibial nerves, but preserved motor nerve conduction velocities. His mother, one brother and one sister reportedly have similar symptoms of peripheral neuropathy but denied further neurophysiological testing or genetic analysis. The point mutation c.1040A>T in exon 11, leading to the exchange of Glutamine to Valine at position 347 (E347V) of the protein, was detected in a 32 year old male (fig. 1c, patient 3). The mutation was not observed by SSCP analysis in over 200 control chromosomes, detection by restriction analysis was not possible. The parents of the patient were reported to be healthy and unrelated, there is no history of peripheral neuropathies in the family. The patient has distal atrophy of his legs since childhood. He also shows high-grade paresis of peroneus muscles in both legs, severe pain in both legs and distal sensory loss. Electrophysiological studies indicate an axonal neuropathy with mildly decreased mNCV. Page 2 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 http://www.biomedcentral.com/1471-2350/7/53 Table 1: Clinical features of patients with MFN2 mutation 1 2 3 4 5 6 58/F 48 weakness in LE 34/F 22 muscle crampi in LE 32/M childhood - 27/F 26 paraesthesia in LE 44/F 6 foot deformities 65/M 62 gait ataxia Motor UE LE 0 2+ 0 2+ 0 2+ 0 2+ 2+ 3+ 0 2+ Sensory pain/touch deep sense 1+ 2+ 1+ 1+ 0 - 0 1+ 2+ 2+ 2+ 2+ normal in UE, decreased (knee), absent (ankle) normal in UE, absent (knee, ankle) normal in UE, absent (ankle) normal in UE, absent (knee, ankle) decreased in UE, absent (knee, ankle) normal in UE, absent (knee, ankle) yes yes yes yes yes yes Age (y)/sex Onset age (y) Initial symptoms Reflexes Pes cavus/varus 0, 1+, 2+, and 3+ = no, minimal, moderate, and severe involvement for muscle weakness and sensory deficit; – = no precise data. UE = upper extremities, LE = lower extremities. Patient 4, a 27 year old female, presented the mutation c.1403G>A in exon 14 (fig. 1d). The mutation leads to the exchange of Arginine to Histidine (R468H). Clinically the patient shows distal weakness and atrophy of the legs, distal sensory loss and decreased mNCV. Her father has Par- kinson disease and distal neuropathy. Her paternal grandfather had pes cavus. Her sister and her mother both do not present any symptoms of neuropathy. Mutation analysis in the parents by restriction with AciI and by sequencing proved the same mutation in her father, indi- Table 2: Nerve conduction study in patients with CMT associated with mutation in MFN2 Normal 1 2 3 4 5 6 ≤ 3,9 ≥ 50 ≥6 2,8 53 11,4 3 50 14,2 n.d. 3,8 46,2 n.d. 5 56 11 n.d. ≤ 4,8 ≥ 42 7,6 37 4 45 not recordable not recordable ≥4 0,8 8,4 ≤ 5,1 ≥ 41 6,2 31 4,2 36 7,1 38 n.d. not recordable not recordable Amplitude (mV) ≥5 0,6 0,4 0,4 Sensory Median nerve NCV (m/s) Amplitude (mV) Sural nerve NCV (m/s) ≥ 47 ≥7 60 13,4 54 11 n.d. 57,7 n.d. 45 20 n.d. ≥ 41 34 not recordable 30 56,5 32 not recordable Amplitude (mV) ≥ 10 7,2 1 n.d. 6 Motor Median nerve DML (ms) NCV (m/s) Amplitude (mV) Peroneal nerve DML (ms) NCV (m/s) Amplitude (mV) Tibial nerve DML (ms) NCV (m/s) not recordable 5,3 47,8 2 DML= distal motor latency; NCV = nerve conduction velocity; n.d. = not determined. Page 3 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 D F*ඎ7*9 http://www.biomedcentral.com/1471-2350/7/53 E GඎT G F*ඎ$5+ F*ඎ$0, GඎA H F F$ඎ7(9 AඎT F*ඎ$9, I FBLQV7/IV insT GඎA GඎA wildtype sequence Figure Electropherograms 1 showing novel mutations in the MFN2 gene detected in this analysis Electropherograms showing novel mutations in the MFN2 gene detected in this analysis. Numbering of nucleotides is according to the open reading frame of the cDNA sequence as deposited in GenBank (GenBank accession no. BC017061). cating cosegregation. However, the mutation was also detected in one of 260 control chromosomes. A 44 year old female patient (patient 5) with symptoms of peripheral neuropathy since the age of six was found to carry a point mutation c.2113G>A in exon 18 (fig. 1e) leading to the exchange of Valine to Isoleucine at position 705 (V705I). No mutation was found in 212 control chromosomes by restriction digest with HinI (Fermentas). Her deceased father and her brother were reported to have similar symptoms, but family members were not available for genetic analysis. Patient 5 shows distal weakness and atrophy of the lower and upper extremities. She has drop feet and steppage gait, absent Achilles' tendon reflexes, distal sensory loss of the lower extremities and decreased sensitivity to vibration of both ankles. Patient 6 carries a frameshift mutation (c.2258_2259insT (L753fs)) in exon 19 (fig. 1f). This frameshift mutation causes a change of the last four amino acids of the open reading frame and leads to an extension of five new amino acids at the end of the protein. By restriction analysis of exon 19 with the enzyme PstI, this mutation was not observed in 200 control chromosomes. Molecular genetic analysis was carried out for this patient at the age of 73 years. There is no family history of peripheral neuropathy but he was analyzed under suspect of CMT2 because of symmetric distal weakness and increased distal paresis of the legs. Discussion We detected MFN2 mutations in 6 patients out of 73 patients with a clinical diagnosis of axonal CMT2, indicating a rate of 8% similar to the findings around 10% up to 20% observed by other groups. None of these mutations has been previously published, and (except the mutation c.1403G→ A in patient 4) none of these has been found in unrelated controls. Our data confirm the findings of dominant mutations in the MFN2 gene to be associated with CMT2A [5]. Recently, mutations in MFN2 have also been linked to two rare forms of hereditary neuropathy, namely HMSN V (with pyramidal signs) [8] and HMSN VI (with optic atrophy) [9]. Our patients with mutations in MFN2 have axonal polyneuropathy without additional symptoms. Severity of symptoms is relatively mild and the rate of clinical progression slow. Although there are several hints linking peripheral neuropathies to the mitochondrial network, the function of mitofusins in peripheral nerves and also the role of MFN2 Page 4 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 http://www.biomedcentral.com/1471-2350/7/53 V273G R274Q Q276R* R280H F284Y E347V K357N H361Y* R364W* M376I T105 M G127V H165D+ T206I* I213T F223L T236M V244M P251A V69F L76P R94W* R94Q 103 261 GTPase R418X* E424G R468H 408 433 C V705I 614 646 TM 724 L753fs 752 757 C + HMSN V (with pyramidal signs) (Zhu et al. 2005) * HMSN VI (with optic atrophy) (Züchner et al.2006) Figure 2 of the MFN2 protein, showing functional domains and published mutations Structure Structure of the MFN2 protein, showing functional domains and published mutations. Mutations described in this paper are underlined. Mutations associated with HMSN V and HMSN VI are marked with + and *, respectively. mutations in the pathogenesis of peripheral neuropathy is only partly understood. Mitochondria are active organelles forming a single dynamic network whose continuity is maintained by a balance of fission and fusion events [10]. In both yeast and drosophila, mitochondrial fusion is controlled by the nuclear-encoded mitochondrial transmembrane GTPase fuzzy onions (Fzo) [11-13]. In humans and mice MFN2 and MFN1, two human homologues of Fzo exist and both are essential for embryonic development and mitochondrial fusion [13]. MFN2 is the second HMSN disease gene directly involved in the maintenance of the mitochondrial network. In contrast to mitofusins, overexpression of ganglioside-induced differentiation associated protein 1 (GDAP1) is interfering with mitochondrial fusion and induces fragmentation of mitochondria, and recessive mutations in GDAP1 have been found in patients with CMT4A [14,15]. MFN2 is localized to the outer mitochondrial membrane. The protein contains two coiled-coil regions flanking a transmembrane segment and a GTPase domain. Functional coiled-coil regions are essential for tethering of mitochondria before fusion [16-18]. An intact GTPase domain is indispensable for the function of mitofusins [12,17,19]. Overall, more than 25 different mutations in MFN2 have been observed up to now in patients with CMT2A, but also HMSN V and HMSN VI. There is cur- rently no explanation for the divergence of phenotypes associated with mutations in MFN2 [5]. Many mutations are predicted to affect the GTPase domain of the protein, but an equal proportion has been detected for the region linking the GTPase domain and the first coiled coil region (see fig. 2). The mutations described up to now seem to cluster in several hotspot regions (aa94, aa236–251, aa273–284, aa357–364), but we have not found any recurrent mutation. Five out of six mutations described in this paper are missense mutations, like the majority of mutations detected in MFN2 up to now [5-8]. Of the five missense mutations, one (G127V) affects the GTPase domain, and two mutations change the region linking the GTPase domain and the first coiled coil region (E347V and M376I). The two other missense mutations (R468H and V705I) are predicted to cause amino acid substitutions between the transmembrane domain and the coiled coil regions (fig. 2). The missense mutation c.1403G→ A (R468H) is the first described in the region between the transmembrane domain and the C-terminal coiled coil region, and was detected in patient 4 and her symptomatic father, indicating cosegregation of mutation and disease. The same substitution was detected in one out of 130 anonymous control samples given by blood donors of different ages assumed to be healthy. Since mild symptoms of CMT2 Page 5 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 may have been missed in a younger blood donor added to the control collective, this does not exclude the substition R468H as pathogenic, but it may also represent a rare sequence variant. Molecular biological studies may be necessary to finally determine the nature of this substitution. Another novel mutation (c.1040A>T) found in patient 3 in our series causes the change of the polar glutamine to the non-polar valine at position 347. This amino acid exchange occurred in a highly conserved region of MFN2. This region is one of the indispensable segment of the protein that might provides binding sites for the assembly [18]. Only one stop mutation, R418X, has been described recently in a patient with CMT6 [9]. Interestingly, the frameshift mutation c.2258_2259insT in our patient 6 would result in a protein only differing by four amino acids and an extension of further five new amino acids at the C-terminus of the protein. This mutation may affect the C-terminal coiled-coil domain at the end of the fzomitofusin domain. Analysis of MFN2 deletion constructs revealed that GTPase-dependent interaction between the N-terminal and C-terminal tails of MFN2 through their coiled-coil domains and a highly conserved domain in the most N-terminal region is essential for mitochondrial fusion [18]. On the other hand it has been suggested that the C-terminus of MFN2 contains determinants required for targeting of the protein to the mitochondrial membrane [20]. http://www.biomedcentral.com/1471-2350/7/53 Competing interests The author(s) declare that they have no competing interests. Authors' contributions KE carried out the molecular genetic studies, KE and MM participated in the sequence alignment and drafted the manuscript. MH participated and assisted in molecular genetic studies and the sequence alignment. MM conceived of the study, and participated in the design. JTE participated in its design and coordination and helped to draft the manuscript. MV, GH and JG made major contributions to the clinical characterisation of the patients. All authors read and approved the final manuscript. Acknowledgements We thank the patients and their families for their cooperation References 1. 2. 3. 4. 5. Further studies of promoter domains in the MFN2 gene will help to clarify if these regions are involved in the development of CMT2. Conclusion 6. We confirmed a significant role of mutations in MFN2 in the pathogenesis of Charcot-Marie-Tooth disease type 2. 7. Abbreviations CMT: Charcot-Marie-Tooth 8. CMT2A: Charcot-Marie-Tooth type 2A 9. GDAP1: ganglioside-induced differentiation associated protein 1 KIF1B: kinesin family member protein 1B 10. MFN2: mitofusin 2 mNCV: motor nerve conduction velocity SSCP: single strand conformation polymorphism 11. 12. Ben Othmane K, Middleton LT, Loprest LJ, Wilkinson KM, Lennon F, Rozear MP, Stajich JM, Gaskell PC, Roses AD, Pericak-Vance MA, et al.: Localization of a gene (CMT2A) for autosomal dominant Charcot-Marie-Tooth disease type 2 to chromosome 1p and evidence of genetic heterogeneity. Genomics 1993, 17(2):370-375. Harding AE, Thomas PK: The clinical features of hereditary motor and sensory neuropathy types I and II. Brain 1980, 103(2):259-280. Kuhlenbäumer G, Young P, Hunermund G, Ringelstein B, Stogbauer F: Clinical features and molecular genetics of hereditary peripheral neuropathies. J Neurol 2002, 249(12):1629-1650. Zhao C, Takita J, Tanaka Y, Setou M, Nakagawa T, Takeda S, Yang HW, Terada S, Nakata T, Takei Y, Saito M, Tsuji S, Hayashi Y, Hirokawa N: Charcot-Marie-Tooth disease type 2A caused by mutation in a microtubule motor KIF1Bbeta. Cell 2001, 105(5):587-597. Züchner S, Mersiyanova IV, Muglia M, Bissar-Tadmouri N, Rochelle J, Dadali EL, Zappia M, Nelis E, Patitucci A, Senderek J, Parman Y, Evgrafov O, Jonghe PD, Takahashi Y, Tsuji S, Pericak-Vance MA, Quattrone A, Battaloglu E, Polyakov AV, Timmerman V, Schröder JM, Vance JM: Mutations in the mitochondrial GTPase mitofusin 2 cause Charcot-Marie-Tooth neuropathy type 2A. Nat Genet 2004, 36(5):449-451. Kijima K, Numakura C, Izumino H, Umetsu K, Nezu A, Shiiki T, Ogawa M, Ishizaki Y, Kitamura T, Shozawa Y, Hayasaka K: Mitochondrial GTPase mitofusin 2 mutation in Charcot-Marie-Tooth neuropathy type 2A. Hum Genet 2005, 116(1-2):23-27. Lawson VH, Graham BV, Flanigan KM: Clinical and electrophysiologic features of CMT2A with mutations in the mitofusin 2 gene. Neurology 2005, 65(2):197-204. Zhu D, Kennerson ML, Walizada G, Züchner S, Vance JM, Nicholson GA: Charcot-Marie-Tooth with pyramidal signs is genetically heterogeneous: families with and without MFN2 mutations. Neurology 2005, 65(3):496-497. Züchner S, De Jonghe P, Jordanova A, Claeys KG, Guergueltcheva V, Cherninkova S, Hamilton SR, Van Stavern G, Krajewski KM, Stajich J, Tournev I, Verhoeven K, Langerhorst CT, de Visser M, Baas F, Bird T, Timmerman V, Shy M, Vance JM: Axonal neuropathy with optic atrophy is caused by mutations in mitofusin 2. Ann Neurol 2006, 59(2):276-281. Nunnari J, Marshall WF, Straight A, Murray A, Sedat JW, Walter P: Mitochondrial transmission during mating in Saccharomyces cerevisiae is determined by mitochondrial fusion and fission and the intramitochondrial segregation of mitochondrial DNA. Mol Biol Cell 1997, 8(7):1233-1242. Hermann GJ, Shaw JM: Mitochondrial dynamics in yeast. Annu Rev Cell Dev Biol 1998, 14:265-303. Hales KG, Fuller MT: Developmentally regulated mitochondrial fusion mediated by a conserved, novel, predicted GTPase. Cell 1997, 90(1):121-129. Page 6 of 7 (page number not for citation purposes) BMC Medical Genetics 2006, 7:53 13. 14. 15. 16. 17. 18. 19. 20. http://www.biomedcentral.com/1471-2350/7/53 Chen H, Detmer SA, Ewald AJ, Griffin EE, Fraser SE, Chan DC: Mitofusins Mfn1 and Mfn2 coordinately regulate mitochondrial fusion and are essential for embryonic development. J Cell Biol 2003, 160(2):189-200. Nelis E, Erdem S, Van Den Bergh PY, Belpaire-Dethiou MC, Ceuterick C, Van Gerwen V, Cuesta A, Pedrola L, Palau F, Gabreels-Festen AA, Verellen C, Tan E, Demirci M, Van Broeckhoven C, De Jonghe P, Topaloglu H, Timmerman V: Mutations in GDAP1: autosomal recessive CMT with demyelination and axonopathy. Neurology 2002, 59(12):1865-1872. Niemann A, Ruegg M, La Padula V, Schenone A, Suter U: Ganglioside-induced differentiation associated protein 1 is a regulator of the mitochondrial network: new implications for Charcot-Marie-Tooth disease. J Cell Biol 2005, 170(7):1067-1078. Koshiba T, Detmer SA, Kaiser JT, Chen H, McCaffery JM, Chan DC: Structural basis of mitochondrial tethering by mitofusin complexes. Science 2004, 305(5685):858-862. Santel A, Fuller MT: Control of mitochondrial morphology by a human mitofusin. J Cell Sci 2001, 114(Pt 5):867-874. Honda S, Aihara T, Hontani M, Okubo K, Hirose S: Mutational analysis of action of mitochondrial fusion factor mitofusin-2. J Cell Sci 2005, 118(Pt 14):3153-3161. Eura Y, Ishihara N, Yokota S, Mihara K: Two mitofusin proteins, mammalian homologues of FZO, with distinct functions are both required for mitochondrial fusion. J Biochem (Tokyo) 2003, 134(3):333-344. Rojo M, Legros F, Chateau D, Lombes A: Membrane topology and mitochondrial targeting of mitofusins, ubiquitous mammalian homologs of the transmembrane GTPase Fzo. J Cell Sci 2002, 115(Pt 8):1663-1674. Pre-publication history The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2350/7/53/prepub Publish with Bio Med Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime." Sir Paul Nurse, Cancer Research UK Your research papers will be: available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright BioMedcentral Submit your manuscript here: http://www.biomedcentral.com/info/publishing_adv.asp Page 7 of 7 (page number not for citation purposes)