Hepatitis B - Bildung — BRK
Werbung

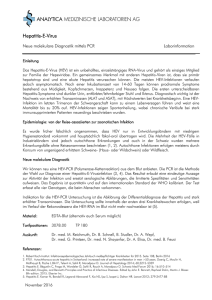
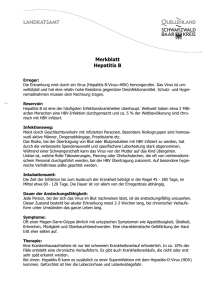
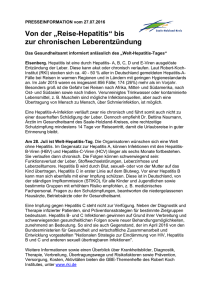
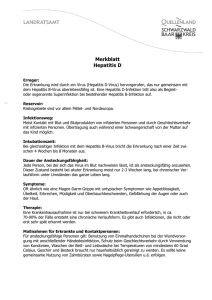
Hepatitis B 1 Hepatitis B Klassifikation nach ICD-10 B16.- Akute Virushepatitis B B16.0 Akute Virushepatitis B mit Delta-Virus (Begleitinfektion) und mit Coma hepaticum B16.1 Akute Virushepatitis B mit Delta-Virus (Begleitinfektion) ohne Coma hepaticum B16.2 Akute Virushepatitis B ohne Delta-Virus mit Coma hepaticum B16.9 Akute Virushepatitis B ohne Delta-Virus und ohne Coma hepaticum B18.0 Chronische Virushepatitis B mit Delta-Virus B18.1 Chronische Virushepatitis B ohne Delta-Virus ICD-10 online (WHO-Version 2011) [1] Die Hepatitis B ist eine Infektionskrankheit der Leber mit dem Hepatitis-B-Virus (HBV), die häufig akut (90 %), gelegentlich auch chronisch verläuft. Mit etwa 350 Millionen chronisch infizierten Menschen ist die Hepatitis B weltweit die häufigste Virusinfektion. Bei etwa einem Drittel der Weltbevölkerung sind als Zeichen einer überstandenen HBV-Infektion Antikörper nachweisbar. Auf Basis der chronischen Leberentzündung kann eine Leberzirrhose, sowie ein Leberzellkarzinom entstehen. Die Therapie einer chronischen Hepatitis B ist schwierig, daher ist die vorbeugende Impfung die wichtigste Maßnahme zur Vermeidung der Infektion und Verminderung der Virusträgerzahl. Erreger Der Erreger der Hepatitis B, das etwa 42 nm große Hepatitis-B-Virus, ist ein partiell doppelsträngiges DNA-Virus und gehört zur Familie der Hepadnaviridae. Zum Vergleich: Rote Blutkörperchen sind mit 7,5 μm ca. 150-mal so groß. Das ca. 3200 bp große Genom ist verpackt in ein ikosaedrisches Kapsid, dem Hepatitis-B-Core-Protein (= HBV-Core-Antigen, HBcAg). Es erfüllt eine ähnliche Funktion wie der Zellkern bei Mehrzellern. Das Kapsid ist von einer Virushülle umgeben, die aus einer zellulären Lipidmembran und eingelagerten Oberflächenproteinen Virionen und leere Partikel des Hepatitis-B-Virus des Virus aufgebaut ist. Von diesen Oberflächenproteinen (HBsAg hepatitis B surface antigen) existieren drei unterschiedlich große Formen (L-, M- und S-HBsAg). Während der Vermehrung des HBV in der Leberzelle wird meist ein weiteres Protein in die Blutbahn abgegeben, das HBV-e-Antigen (HBeAg, „e“ wird als „exkretorisch“ gedeutet, ein Antigen ist in der Medizin ein von den Abwehrzellen als fremd erkanntes Molekül); das HBeAg ist ein frisch produziertes, dann gekürztes Hepatitis-B-Core-Protein (HBcAg), das vom Virus ins Blut abgegeben wird. Die meisten der Oberflächenproteine im Blut sind nicht am Aufbau der infektiösen Viren beteiligt (der sogenannten Dane-Partikel), sondern liegen als Filamente oder sphärische Partikel ohne Kapsid und DNA vor (bis zu 600 μg/ml HBs-Protein). Es sind etwa 10.000-mal mehr „leere“ HBsAg-Partikel im Blut als komplette HBV-Partikel nachweisbar; dies hat wichtige Konsequenzen für den Krankheitsverlauf. Die Partikel lenken das Immunsystem ab, ähnlich einem Raketenabwehrsystem bei Flugzeugen. Dafür helfen sie bei der Diagnostik der Hepatitis. Die Therapie ist so schwierig, weil die Viren ihre Erbinformation in die DNA der Leberzelle schreiben. Dafür nutzen sie RNA-Zwischenstufen und ähnlich dem HI-Virus Reverse Transkriptasen; das HBV ist daher eng mit den echten Hepatitis B Retroviren verwandt. Eine Elimination des Hepatitis-B-Virus aus dem Organismus ist nicht möglich, die Viren-DNA ist fester Bestandteil der DNA der Leberzellen und teilt sich mit diesen. Nach überstandener akuter Infektion geht es in einen Ruhezustand über, aus dem es bei einer Immunschwäche (z.B. nach Organtransplantationen, Chemotherapie oder bei HIV-Infektion) reaktiviert wird. Wegen der Ähnlichkeit zu Retroviren sind einige Arzneistoffe sowohl gegen HIV als auch Hepatitis B wirksam (die Nukleosidische Reverse-Transkriptase-Inhibitoren Lamivudin und Adefovir). Die RNA-Zwischenstufe macht HBV für ein DNA-Virus ungewöhnlich anpassungsfähig. Es bildet leicht Varianten (sogenannte Quasispezies), die das Immunsystem unterlaufen oder gegen antivirale Medikamente resistent sind. Vom HBV sind acht Genotypen (A–H) bekannt, die geographisch unterschiedlich verteilt sind. Verbreitung Das HBV kommt weltweit vor. Es ist endemisch in China, Südostasien, dem Nahen und Mittleren Osten, der Türkei und in Teilen Afrikas. Dank der seit einigen Jahren durchgeführten Impfkampagnen ist das Vorkommen chronischer Virusträger in Nord- und Westeuropa, USA, Kanada, Mexiko und südlichen Regionen Südamerikas auf unter 1 % gefallen. In Deutschland sind 0,3 bis 0,8 % der Bevölkerung Verbreitung Hepatitis B (Stand 2005) HBs-Antigen-positiv, d. h. 250.000 bis 650.000 sind chronische █ Hoch: Prävalenz höher als 8% █ Mittel : zwischen 2% und 7% Virusträger. Offiziell werden in Deutschland etwa 5000 █ Niedrig : weniger als 2% Neuinfektionen pro Jahr gemeldet, wobei die wirkliche Zahl wesentlich höher anzusetzen ist. Gehäuft ist in Deutschland eine Trägerschaft bei intravenös Drogenabhängigen, Homosexuellen und Personen aus dem arabischen Raum und der Türkei (hier oft angeborene Infektionen) zu finden. Übertragung Die Infektion mit HBV erfolgt parenteral und sexuell, d. h. durch Blut oder andere Körperflüssigkeiten eines infizierten, HBsAg-positiven Patienten. Die Infektiosität eines Virusträgers ist abhängig von der Viruskonzentration im Blut; bei sogenannten hochvirämischen Trägern (107 bis zu 1010 HBV-Genome/ml) finden sich infektiöse Viren auch in Urin, Speichel, Samenflüssigkeit, Tränensekret, Galle und Muttermilch. Die Eintrittspforten sind meist kleinste Verletzungen der Haut oder Schleimhaut. Daher gilt als Risikofaktor auch der ungeschützte Geschlechtsverkehr. Unter Kleinkindern kann die Infektion auch durch Kratzen oder Beißen weitergegeben werden. Auch Gegenstände des täglichen Lebens, wie zum Beispiel Rasierapparate oder Nagelscheren, mit denen man sich häufig geringfügig verletzt, können das HBV übertragen. In Ländern, in denen noch das Rasieren beim Barbier weit verbreitet ist, findet sich meist auch eine erhöhte Häufigkeit von HBV-Infektionen. Weitere wichtige Übertragungsmöglichkeiten sind auch größere Verletzungen mit Blutkontakt z. B. bei intravenösem Drogenkonsum, Tätowierung und Piercing. Im medizinischen Bereich kann HBV durch invasive, operative Eingriffe und Verletzungen übertragen werden, so von unerkannten HBsAg-Trägern auf Patienten oder von nicht-getesteten Patienten auf medizinisches oder zahnärztliches Personal. Die Übertragung von HBV durch Blut und Blutprodukte bei einer Transfusion ist seit der Testung von Blutspenden auf anti-HBc, HBsAg und HBV-DNA in Deutschland sehr selten geworden. In Endemiegebieten ist der wichtigste Übertragungsweg die vertikale Infektion von einer HBsAg-positiven Mutter unter der Geburt (perinatal) auf das Kind. Die perinatale Infektion hat zu 90 % eine chronische Infektion des Kindes zur Folge. Das Risiko einer Ansteckung durch eine Nadelstichverletzung mit bekannt HBsAg-positivem Indexpatient liegt bei etwa 10–30 %. Dieses Risiko ist sehr abhängig von der Viruskonzentration, unterhalb von 105 HBV-Genomen/ml ist 2 Hepatitis B eine solche Übertragung im medizinischen Bereich nicht nachgewiesen worden. Diese z. B. in Großbritannien bereits festgelegte Grenze hat große Bedeutung bei der Beschäftigung von HBsAg-Trägern im medizinischen Bereich. Klinischer Verlauf Akute Hepatitis B Etwa 2/3 aller Infektionen verlaufen ohne klinische Anzeichen (asymptomatisch), d. h. nur etwa ein Drittel der Infizierten zeigen nach einer Inkubationszeit von ein bis sechs Monaten die klassischen Hepatitiszeichen wie Gelbfärbung der Haut und der Skleren (Ikterus), dunklen Urin, Gliederschmerzen, Schmerzen im Oberbauch, Übelkeit, Erbrechen und Durchfall. Häufig wird nach asymptomatischen Verläufen eine leichte Abgeschlagenheit angegeben oder eine Erhöhung der Leberenzyme (Transaminasen) wird zufällig entdeckt; eine solche Infektion kann meist nur durch die Serologie erkannt werden. In der Regel heilt eine unkomplizierte akute Hepatitis B nach zwei bis sechs Wochen klinisch aus, der Nachweis von Antikörpern gegen das HBsAg (anti-HBs) zeigt dies an. Mit dem Verschwinden des HBsAg und dem Auftauchen von anti-HBs (Serokonversion) gilt die Ansteckungsgefahr als überwunden. Selten kann eine akute Hepatitis B einen schwereren Verlauf nehmen, bei dem es zu einer Beeinträchtigung der Blutgerinnung und zu Schädigungen des Gehirns (Enzephalopathie) kommt; hier wird eine Therapie mit einem Nukleosidanalogon (z. B. Lamivudin) empfohlen. Im schwersten Fall kommt es bei ca. 1 % der symptomatischen Verläufe zu lebensbedrohlichen Verlauf (in Stunden bis wenige Tage), der sogenannten fulminanten Hepatitis. In diesem Fall gelten das rasche Verschwinden des HBsAg und eine Schrumpfung der Leber als ungünstige Zeichen; eine medikamentöse Therapie und intensivmedizinische Betreuung mit der Möglichkeit einer Lebertransplantation sind geboten. Die Verabreichung von Interferon ist bei jeder Form der akuten Hepatitis B kontraindiziert. Chronische Hepatitis B In vielen Fällen verläuft auch die Infektion unbemerkt und ohne Symptome. Definitionsgemäß spricht man von einer chronischen Hepatitis B, wenn die Symptome einer durch HBV verursachten Leberentzündung sowie entsprechende viralen Marker länger als sechs Monate bestehen (persistieren). Chronisch verläuft diese Erkrankung in 5–10 % der Fälle. Sie kann sich entweder im Anschluss an eine akute Hepatitis B entwickeln oder auch primär chronisch verlaufen. Die Chronifizierungsrate nimmt mit sinkendem Alter stetig zu und ist bei Neugeborenen am höchsten. Diese werden bei einer Infektion wie oben beschrieben in über 90 % der Fälle zu chronischen Virusträgern. Noch bei vierjährigen Patienten verläuft die Hälfte aller Infektionen chronisch. Bei etwa einem Viertel aller chronischen Hepatitis-B-Erkrankungen ist ein sich im Schweregrad steigernder Krankheitsverlauf (progredienter) zu beobachten, der dann häufig zu erheblichen Folgeschäden wie beispielsweise zu einem Leberzellkarzinom oder Leberzirrhose führt. Spätestens bei Auftreten von Bewusstseinsveränderungen (sogenannte Hepatische Enzephalopathie) ist die Verlegung in ein Zentrum für Lebererkrankungen angebracht. Bis zu 25 % der Erkrankten sterben an den Folgekrankheiten des HBV (Leberzirrhose, Leberzellkarzinom). Etwa 5 % der HBV-Infizierten sind zusätzlich an Hepatitis D erkrankt. HBV gehört zusammen mit dem Epstein-Barr-Virus (EBV), dem Hepatitis-C-Virus (HCV), dem humanen Papillomvirus (HPV), Humanen T-lymphotropen Virus 1 (HTLV-1) und dem Humanen Herpesvirus 8 (HHV-8, auch Kaposi-Sarkom-Herpesvirus, KSHV) zu einer Gruppe von humanen Viren, die weltweit für 10 bis 15 Prozent aller Krebserkrankungen verantwortlich sind.[2] 3 Hepatitis B Reaktivierung Durch neue Therapien bei der Behandlung von Leukämie und zur Immunsuppression nach einer Organtransplantation wurde in den letzten Jahren in einzelnen Fällen eine Reaktivierung einer alten, klinisch ausgeheilten HBV-Infektion beobachtet. Auch wurden Reaktivierungen von HBV bei AIDS im fortgeschrittenen Stadium (C3) beschrieben. Die HBV-Infektion lag in einigen Fällen der Reaktivierung bereits Jahrzehnte zurück, und die Patienten hatten vorher das klassische serologische Muster einer alten Infektion (anti-HBc und anti-HBs positiv, siehe Diagnostik). Eine solche Reaktivierung verläuft oft sehr schwer, insbesondere wenn nach erfolgter Reaktivierung die Immunsuppression reduziert wird und durch die dann erfolgende Immunabwehr die Leber wie bei einer fulminanten Hepatitis rasch zerstört wird. Das Auftauchen solcher Symptome nach Reduzierung der Immunsuppression (z. B. bei Beendigung einer Chemotherapie oder bei erfolgreicher HIV-Therapie) wird auch Immunrekonstitutions-Syndrom genannt. Durch eine Reaktivierung besonders gefährdet sind Patienten nach Nierentransplantation, Knochenmark-Transplantation und Patienten mit Akuter Myeloischer Leukämie. Eine Behandlung mit einem Nukleosidanalogon für mehrere Wochen bis Monate ist bei einer nachgewiesenen Reaktivierung geboten. Das Phänomen einer Reaktivierung verdeutlicht noch einmal die Tatsache, dass das HBV ähnlich wie ein echtes Retrovirus in einen Ruhezustand übergehen kann und nicht aus allen Zellen eliminiert wird. Insgesamt ist die Reaktivierung jedoch ein sehr seltenes Ereignis. Diagnose Man unterscheidet bei der Hepatitis B hauptsächlich zwei Verlaufsformen, die akute Hepatitis B, die nach spätestens einem halben Jahr völlig ausgeheilt ist, und die chronische Hepatitis B. Die chronische Hepatitis B entsteht aus einer nicht ausgeheilten akuten, kann jahrzehntelang dauern und eine Leberzirrhose oder ein Hepatozelluläres Carcinom (HCC) zur Folge haben. Die Sicherung der jeweiligen Diagnose erfolgt über drei Hauptbestandteile, nach denen gesucht wird: • Virus-Antigene (also das Virus selbst oder dessen Eiweißstoffe): Findet man noch Virus-Antigene (HBs-Ag, HBe-Ag), dann ist die Infektion nicht überstanden: Es wird eine akute oder chronische Hepatitis B vorliegen oder, im günstigsten Fall, wenn nur HBs-Ag nachweisbar ist und der Patient sonst gesund ist, ein sog. HBs-Träger-Status. Patienten mit HBe-Ag im Blut sind hoch ansteckend; aber auch bei alleinigem HBs-Ag im Blut besteht Ansteckungsgefahr. • Antikörper (die unsere Abwehr dagegen bildet): Anti-HBs sind Zeichen einer Ausheilung. Man findet sie auch nach erfolgreicher Hepatitis-B-Impfung. Sie zeigen also eine Immunität gegen Hepatitis B an. Anti-HBc-IgM sprechen für das Vorliegen einer akuten Hepatitis. Anti-HBc-IgG findet man sowohl im späteren akuten Stadium wie auch nach Abheilung. Anti-HBe können in der Heilungsphase einer akuten Hepatitis auftreten. Ihr Auftreten bei chronischer Hepatitis zeigt eine Verbesserung und eine verminderte Ansteckungsgefahr an. • Virus-DNA (Desoxyribonukleinsäure, also Erbsubstanz des Virus): Früher hat man die DNA-Messung bei Hepatitis B zur Diagnose unklarer Fälle und zur Abschätzung der Ansteckungsgefahr eingesetzt. Heute ist die Messung auch für die Diagnose und Beobachtung der chronischen Hepatitis wichtig. Wenig Virus-DNA im Blut spricht für eine ruhende Infektion, viel DNA für eine aktive chronische Hepatitis. Tabelle 1: Häufige serologische Konstellationen und ihre diagnostische Interpretation (für die jeweilige Diagnosestellung nicht notwendige Parameter sind eingeklammert) 4 Hepatitis B 5 anti-HBc anti-HBs HBs-Antigen anti-HBe HBe-Antigen HBV-DNA Interpretation neg. pos. (neg.) (neg.) (neg.) (neg.) Z.n. Impfung, >100 mIU anti-HBs/ml: Immunität 10-100 mIU/ml: relativer Schutz, Auffrischung empfohlen pos. pos. (neg.) (neg./pos.) (neg.) (neg.) Alte, klinisch ausgeheilte Infektion pos. (neg.) pos. neg. pos. hochpos. pos. (neg.) pos. pos. neg. pos. pos. (neg.) pos. neg. neg. hochpos. Hochvirämische Infektion Niedrigvirämische Infektion „HBe-Minus-Mutante“, prä-Core-Mutation Tabelle 2: Seltene serologische Konstellationen , die einer Überprüfung in einem Speziallabor bedürfen anti-HBc anti-HBs HBs-Antigen anti-HBe HBe-Antigen HBV-DNA Interpretation pos. neg. neg. neg. neg. neg. „Isolierte anti-HBc-Positivität“: unspezifische Testreaktion oder sehr alte, ausgeheilte Infektion pos. neg. neg. pos. neg. neg. Sehr alte, ausgeheilte Infektion mit Verlust des anti-HBs neg. pos. pos. neg. neg. neg. Meist unspezifische Testreaktion des HBsAg-Tests oder sehr seltener Befund wenige Tage nach einer wiederholten Impfung neg. neg. pos. neg. neg. pos. fehlendes anti-HBc: Häufige Konstellation bei Infektion eines Nicht-Immunkompetenten oder bei angeborener Infektion Therapie Im Akutstadium (d. h. in den ersten Monaten nach der Infektion) wird eine Hepatitis B gewöhnlich nur symptomatisch therapiert, da die Erkrankung in 90–95 % der Fälle von selbst ausheilt. Für eine chronische Hepatitis B stehen zwei Medikamentenklassen zur Verfügung: 1. pegyliertes Interferon (Peginterferon α), welches einmal wöchentlich gespritzt wird. Interferone regen das Immunsystem an, damit dieses effektiver gegen das Virus kämpft. 2. Nukleosid- bzw. Nukleotidanaloga, die täglich als Tablette eingenommen werden. Dazu gehören Lamivudin, Adefovir, Entecavir, Telbivudin und Tenofovir. Diese Wirkstoffe behindern das Virus bei der Vermehrung. Weitere Wirkstoffe werden in Studien geprüft. Diese Therapien sind allerdings nicht kurativ, es ist also keine vollständige Heilung zu erwarten. Das Therapieziel ist vielmehr, den Verlauf der chronischen Hepatitis B abzumildern und das Risiko von Spätfolgen zu senken. Selten (bis zu 3 %) kann unter der Therapie mit (Peg-)Interferon oder den anderen Wirkstoffen auch das HBsAg aus dem Blut verschwinden und als Immunreaktion anti-HBs-Antikörper auftreten, was einer Heilung gleichkommt. Welcher Patient wann therapiert werden muss und mit welchem Medikament, ist von Fall zu Fall unterschiedlich. Bei sehr mildem Verlauf wird eine chronische Hepatitis B meist nur beobachtet. Bei Hinweisen auf eine Schädigung der Leber oder anderen Risikofaktoren ist eine Therapie jedoch sehr wichtig (Stand: August 2008). Dies sollte im Einzelfall fachärztlich beurteilt werden. Hepatitis B Impfung Gegen Hepatitis B kann aktiv und passiv geimpft werden. Die aktive Impfung besteht aus einem nachgebauten Bestandteil der Virushülle, dem HBs-Antigen. Aktiv wird der Körper, der gegen die Fremdstoffe Abwehrmoleküle (Immunglobuline) bildet, um sie zu zerstören. Nach 3 Impfungen kennen die Immunzellen den Virusbestandteil und können es bei einer echten Infektion bekämpfen. Entgegen anderen Meinungen werden bei der Hepatitis-B-Impfung keine echten Viren verabreicht. Die Anzahl der Non-Responder ist deutlich unter 10 %. Die Impfung wird dreimal durchgeführt: 1. Impfung (Woche 0) 2. Impfung (ca. 1 Monat später) 3. Impfung (ein halbes Jahr bis 1 Jahr nach erster Impfung) Zwei Wochen nach der dritten Impfung besteht Impfschutz für mindestens zehn Jahre. Je nach Impftiter, der Anzahl der noch aktiven Hepatitis Abwehrmoleküle, sollte nun eine Auffrischimpfung gemacht werden.[3] Bei der passiven Impfung werden Hyperimmunoglobuline gespritzt; fertige Immunglobuline, die dem Immunsystem helfen, die Viren zu bekämpfen. Diese wird zusammen mit aktivem Impfstoff nach Kontakt mit infiziertem Material (medizinisch Postexpositionsprophylaxe, bes. im Krankenhaus: Nadelverletzungen, Schleimhautkontakt, etc.) und bei Neugeborenen von Hep-B positiven Müttern bis 12 h nach Kontakt bzw. Geburt verabreicht.[4] Dieser Impfschutz wird bei Neugeborenen nach dem normalen Impfschema (0. - 1. - 6. Monat) vervollständigt. Damit wird eine Immunantwort bei über 95% der Impflinge erreicht. Da man sich nur mit Hepatitis D anstecken kann, wenn schon eine Hepatitis B vorliegt, schützt die Hepatitis-B-Impfung auch vor Hepatitis-D-Viren. Darüber hinaus gibt es einen Kombinationsimpfstoff, der auch gegen Hepatitis A schützt. Generell wird die Impfung gut vertragen. Gelegentlich kommt es zu Rötungen an der Impfstelle. Seltener sind Fieber, Kopfschmerzen, Abgeschlagenheit und Gelenkbeschwerden. Impfschäden oder schwere allergische Reaktionen sind sehr selten. Ein ursächlicher Zusammenhang mit neurologischen Erkrankungen (z. B. Guillain-Barré-Syndrom) ist bislang ungeklärt; es liegen Einzelfallberichte vor, bei denen ein zufälliges zeitliches Zusammentreffen vermutet wird (Cornberg et al., Leitlinien der DGVS 2007). Wenn akute Erkrankungen oder andere Kontraindikationen vorliegen, z.B. ein Bestandteil des Impfstoffs nicht vertragen wird oder eine fieberhafte Erkrankung, sollte man auf die Impfung verzichten (Cornberg 2007). Ob eine unsymptomatische Multiple Sklerose durch die HBV-Impfung ausgelöst werden kann, wurde wiederholt in Studien und Einzelfallberichten diskutiert. Es ist bislang aber nicht wissenschaftlich belegt (Cornberg 2007). Eine Studie von Hernán et al (Neurology 2004) konnte angeblich ein dreifach erhöhtes MS-Risiko durch die HBV-Impfung feststellen; sie wurde aber (u. a. von der Weltgesundheitsorganisation WHO) wegen methodischer Fehler als irreführend und nicht aussagekräftig kritisiert: Bei der Studie wurden nicht etwa Gesunde befragt, wie viele von ihnen nach der Impfung an MS erkrankten, sondern MS-Patienten, wie viele von ihnen in den drei Jahren vor ihrer MS-Diagnose gegen Hepatitis B geimpft wurden (dies traf nur auf 11 von ursprünglich 713 MS-Patienten zu). Die Weltgesundheitsorganisation forderte 1992 alle Mitgliedsstaaten dazu auf, die Hepatitis-B-Impfung in nationale Routineimpfprogramme aufzunehmen.[5] In Taiwan hat die universelle HBV-Impfung die Rate an Leberkrebs erheblich gesenkt.[6] Deutschland Eine Impfung (aktive Immunisierung) wird bei allen Säuglingen und Kindern von der Ständigen Impfkommission (StIKo) empfohlen, und zwar seit 1995[7]. Außerdem sollten Personen in Heil- und Pflegeberufen sowie Bestatter, Thanatologen und Leichenwäscher, Mitarbeiter in der Pathologie, Dialysepatienten, Promiskuitive, Drogenabhängige und Reisende in Risikogebiete nicht auf den Impfschutz verzichten.[3] Die Hepatitis-B-Impfung ist Kassenleistung bei Kindern und Jugendlichen; bei Erwachsenen erstatten einige Kassen die Kosten einer 6 Hepatitis B Reiseimpfung als Satzungsleistung. Österreich In Österreich wird die Grundimmunisierung bei allen Säuglingen ab dem dritten Lebensmonat – in der Regel mit einem sechsfach kombinierten Impfstoff – durchgeführt, ansonsten wird bei den bislang ungeimpften Kindern die Grundimmunisierung im Rahmen der Schulimpfung im elften Lebensjahr durchgeführt. Es wird angenommen, dass nach einer kompletten Grundimmunisierung (bei Respondern) der Schutz vor Komplikationen einer Hepatitis-B-Infektion durch die Reaktivierung der spezifischen Gedächtniszellen gewährleistet ist, auch wenn die Impfantikörper verschwunden sind.[8] Auf die Schulimpfung gegen Hepatitis B dürfte somit verzichtet werden, wenn die ersten geimpften Säuglinge dieses Alter erreicht haben, da bei jungen Impflingen eine spätere Auffrischungsimpfung derzeit von Experten nicht empfohlen wird. Einzelnachweise [1] http:/ / www. dimdi. de/ static/ de/ klassi/ diagnosen/ icd10/ htmlamtl2011/ index. htm [2] Martin, D. and Gutkind J. S.: Human tumor-associated viruses and new insights into the molecular mechanisms of cancer. In: Oncogene. 27, Nr. 2, 2008, S. 31-42. PMID 19956178. [3] Impfkalender (http:/ / www. rki. de/ cln_160/ nn_1493664/ DE/ Content/ Infekt/ Impfen/ STIKO/ Empfehlungen/ Aktuelles/ Impfkalender,templateId=raw,property=publicationFile. pdf/ Impfkalender. pdf''STIKO). Epidemiologisches Bulletin Nr.30 des RKI, 27. Juli 2009 [4] H.Renz-Polster, S.Krautzig: Basislehrbuch Innere Medizin 4. Auflage, 2006, S.649 ff [5] World Health Organization: Programmes and Projects: Hepatitis B. (http:/ / www. who. int/ nuvi/ hepb/ en/ ) (englisch) [6] Chang MG et.al. Decreased Incidence of Hepatocellular Carcinoma in Hepatitis B Vaccinees: A 20-Year Follow-up Study. J Natl Cancer Inst. 2009 Sep 16. PMID 19759364 [7] http:/ / www. frauenaerzte-im-netz. de (http:/ / www. frauenaerzte-im-netz. de/ de_hepatitis-impfung-schutzma-nahmen_731. html) [8] Hepatitis-B-Impfung: Genügt die Dauer des Impfschutzes, um eine Impfung im Säuglingsalter in Betracht zu ziehen? nach „Medecine et Enfance“ 2001 (http:/ / www. swiss-paediatrics. org/ paediatrica/ vol12/ n2/ hepbprot-ge. htm) Literatur • Baruch S. Blumberg: Hepatitis B: the hunt for a killer virus. Princeton 2002. Weblinks • Hepatitis B (http://www.kindergesundheit-info.de/610.0.html) Informationsangebot der Bundeszentrale für gesundheitliche Aufklärung • Hepatitis B (http://www.rki.de/DE/Content/InfAZ/H/HepatitisB/HepatitisB.html) – Informationen des Robert Koch-Instituts • Kompetenznetz Hepatitis (http://www.hep-net.de) • Consensus-Leitlinien der DGVS (2007) zur Prophylaxe, Diagnostik und Therapie der Hepatitis B (http://www. dgvs.de/media/Hepatitis_B_Leitlinien_06.2007.pdf) (PDF-Datei; 793 kB) • Laborlexikon: Hepatitis B-Diagnostik (http://www.laborlexikon.de/Lexikon/Infoframe/h/ Hepatitis-B-Diagnostik.htm) • Therapie der HBV-Infektion (http://www.uni-duesseldorf.de/gahepinf/hepatitis/hep_b.htm) • Impfempfehlung des Deutschen Internistenverbandes (http://www.internisten-im-netz.de/de_hepatitis-b_607. html) • Prophylaxe, Diagnostik und Verlauf der Hepatitis-B-Virus-(HBV)-Infektion(AWMF) (http://www. uni-duesseldorf.de/AWMF/ll/021-011.htm) 7 Quelle(n) und Bearbeiter des/der Artikel(s) Quelle(n) und Bearbeiter des/der Artikel(s) Hepatitis B Quelle: http://de.wikipedia.org/w/index.php?oldid=98456148 Bearbeiter: .eXotech, 24-online, A.Savin, A1bi, Aholtman, Andante, Armin P., Avoided, B-Navigator, BKSlink, Baumfreund-FFM, Bertonymus, BurghardRichter, Complex, Cronox, Crux, DasBee, Der Lange, DerHexer, Diba, Dr. Hagemann, Drahreg01, Dschafar, Dundak, Ejka, Etraetra, Felistoria, Felix Stember, Fixi, Flacus, Gerbil, Gilliamjf, Gleiberg, GrandpaScott, Grindinger, Hahnenkleer, Halbarath, Hans J. Castorp, Hardenacke, Hermannthomas, Hoosic06, Howwi, Hubertl, Icarus523, Ingwer22, Inkowik, Iste Praetor, JHeuser, JRG, Jackalope, Jaellee, Jaer, Janpol, Jivee Blau, Johnny Controletti, Jojaju, Judo123, Juliabackhausen, JøMa, Kaisersoft, Klapper, Koethnig, KriSte Mühe, Kubrick, LKD, Lagaly de, Laza, Lennibert, Logograph, Lysozym, MFM, Mager, Magnummandel, Manbu, Martin Bahmann, Martin1978, Matthias2008, Meister-Lampe, Mnh, MoLa, NEUROtiker, Necrophorus, Neokortex, Neun-x, Nothere, Nowadays, O.Koslowski, OecherAlemanne, Olei, OsGr, Ot, Pendulin, Philipp Wetzlar, Pill, Pittimann, Programmajr, Rabauz, Regi51, Reinhard Kraasch, Ritziandreas, Robodoc, S.lukas, Schweinebrot, Seehundnz, Seelo2010, Sinn, Solotoj, Spuk968, StYxXx, Stadtvogel70, Stepsen, Stoll, Strolch1983, THWZ, Template namespace initialisation script, Torte92, Totenmontag, Trockennasenaffe, Tschäfer, Uwe Gille, Video2005, Vigilius, Westiandi, WikiMM, Wnme, ³²P, 201 anonyme Bearbeitungen Quelle(n), Lizenz(en) und Autor(en) des Bildes Datei:Hepatitis B virus 01.jpg Quelle: http://de.wikipedia.org/w/index.php?title=Datei:Hepatitis_B_virus_01.jpg Lizenz: Public Domain Bearbeiter: Original uploader was MarcoTolo at en.wikipedia Datei:HBV_prevalence_2005.svg Quelle: http://de.wikipedia.org/w/index.php?title=Datei:HBV_prevalence_2005.svg Lizenz: Creative Commons Attribution-Sharealike 3.0,2.5,2.0,1.0 Bearbeiter: Nanoxyde Lizenz Wichtiger Hinweis zu den Lizenzen Die nachfolgenden Lizenzen bezieht sich auf den Artikeltext. Im Artikel gezeigte Bilder und Grafiken können unter einer anderen Lizenz stehen sowie von Autoren erstellt worden sein, die nicht in der Autorenliste erscheinen. Durch eine noch vorhandene technische Einschränkung werden die Lizenzinformationen für Bilder und Grafiken daher nicht angezeigt. An der Behebung dieser Einschränkung wird gearbeitet. Das PDF ist daher nur für den privaten Gebrauch bestimmt. Eine Weiterverbreitung kann eine Urheberrechtsverletzung bedeuten. Creative Commons Attribution-ShareAlike 3.0 Unported - Deed Diese "Commons Deed" ist lediglich eine vereinfachte Zusammenfassung des rechtsverbindlichen Lizenzvertrages (http:/ / de. wikipedia. org/ wiki/ Wikipedia:Lizenzbestimmungen_Commons_Attribution-ShareAlike_3. 0_Unported) in allgemeinverständlicher Sprache. Sie dürfen: • das Werk bzw. den Inhalt vervielfältigen, verbreiten und öffentlich zugänglich machen • Abwandlungen und Bearbeitungen des Werkes bzw. Inhaltes anfertigen Zu den folgenden Bedingungen: • • Namensnennung — Sie müssen den Namen des Autors/Rechteinhabers in der von ihm festgelegten Weise nennen. Weitergabe unter gleichen Bedingungen — Wenn Sie das lizenzierte Werk bzw. den lizenzierten Inhalt bearbeiten, abwandeln oder in anderer Weise erkennbar als Grundlage für eigenes Schaffen verwenden, dürfen Sie die daraufhin neu entstandenen Werke bzw. Inhalte nur unter Verwendung von Lizenzbedingungen weitergeben, die mit denen dieses Lizenzvertrages identisch, vergleichbar oder kompatibel sind. Wobei gilt: • • Verzichtserklärung — Jede der vorgenannten Bedingungen kann aufgehoben werden, sofern Sie die ausdrückliche Einwilligung des Rechteinhabers dazu erhalten. Sonstige Rechte — Die Lizenz hat keinerlei Einfluss auf die folgenden Rechte: • • • • Die gesetzlichen Schranken des Urheberrechts und sonstigen Befugnisse zur privaten Nutzung; Das Urheberpersönlichkeitsrecht des Rechteinhabers; Rechte anderer Personen, entweder am Lizenzgegenstand selber oder bezüglich seiner Verwendung, zum Beispiel Persönlichkeitsrechte abgebildeter Personen. Hinweis — Im Falle einer Verbreitung müssen Sie anderen alle Lizenzbedingungen mitteilen, die für dieses Werk gelten. Am einfachsten ist es, an entsprechender Stelle einen Link auf http:/ / creativecommons. org/ licenses/ by-sa/ 3. 0/ deed. de einzubinden. Haftungsbeschränkung Die „Commons Deed“ ist kein Lizenzvertrag. Sie ist lediglich ein Referenztext, der den zugrundeliegenden Lizenzvertrag übersichtlich und in allgemeinverständlicher Sprache, aber auch stark vereinfacht wiedergibt. Die Deed selbst entfaltet keine juristische Wirkung und erscheint im eigentlichen Lizenzvertrag nicht. GNU Free Documentation License Version 1.2, November 2002 Copyright (C) 2000,2001,2002 Free Software Foundation, Inc. 51 Franklin St, Fifth Floor, Boston, MA 02110-1301 USA Everyone is permitted to copy and distribute verbatim copies of this license document, but changing it is not allowed. 0. PREAMBLE The purpose of this License is to make a manual, textbook, or other functional and useful document "free" in the sense of freedom: to assure everyone the effective freedom to copy and redistribute it, with or without modifying it, either commercially or noncommercially. Secondarily, this License preserves for the author and publisher a way to get credit for their work, while not being considered responsible for modifications made by others. This License is a kind of "copyleft", which means that derivative works of the document must themselves be free in the same sense. It complements the GNU General Public License, which is a copyleft license designed for free software. We have designed this License in order to use it for manuals for free software, because free software needs free documentation: a free program should come with manuals providing the same freedoms that the software does. But this License is not limited to software manuals; it can be used for any textual work, regardless of subject matter or whether it is published as a printed book. We recommend this License principally for works whose purpose is instruction or reference. 1. APPLICABILITY AND DEFINITIONS This License applies to any manual or other work, in any medium, that contains a notice placed by the copyright holder saying it can be distributed under the terms of this License. Such a notice grants a world-wide, royalty-free license, unlimited in duration, to use that work under the conditions stated herein. The "Document", below, refers to any such manual or work. Any member of the public is a licensee, and is addressed as "you". You accept the license if you copy, modify or distribute the work in a way requiring permission under copyright law. A "Modified Version" of the Document means any work containing the Document or a portion of it, either copied verbatim, or with modifications and/or translated into another language. A "Secondary Section" is a named appendix or a front-matter section of the Document that deals exclusively with the relationship of the publishers or authors of the Document to the Document's overall subject (or to related matters) and contains nothing that could fall directly within that overall subject. (Thus, if the Document is in part a textbook of mathematics, a Secondary Section may not explain any mathematics.) The relationship could be a matter of historical connection with the subject or with related matters, or of legal, commercial, philosophical, ethical or political position regarding them. The "Invariant Sections" are certain Secondary Sections whose titles are designated, as being those of Invariant Sections, in the notice that says that the Document is released under this License. If a section does not fit the above definition of Secondary then it is not allowed to be designated as Invariant. The Document may contain zero Invariant Sections. If the Document does not identify any Invariant Sections then there are none. The "Cover Texts" are certain short passages of text that are listed, as Front-Cover Texts or Back-Cover Texts, in the notice that says that the Document is released under this License. A Front-Cover Text may be at most 5 words, and a Back-Cover Text may be at most 25 words. A "Transparent" copy of the Document means a machine-readable copy, represented in a format whose specification is available to the general public, that is suitable for revising the document straightforwardly with generic text editors or (for images composed of pixels) generic paint programs or (for drawings) some widely available drawing editor, and that is suitable for input to text formatters or for automatic translation to a variety of formats suitable for input to text formatters. A copy made in an otherwise Transparent file format whose markup, or absence of markup, has been arranged to thwart or discourage subsequent modification by readers is not Transparent. An image format is not Transparent if used for any substantial amount of text. A copy that is not "Transparent" is called "Opaque". Examples of suitable formats for Transparent copies include plain ASCII without markup, Texinfo input format, LaTeX input format, SGML or XML using a publicly available DTD, and standard-conforming simple HTML, PostScript or PDF designed for human modification. Examples of transparent image formats include PNG, XCF and JPG. Opaque formats include proprietary formats that can be read and edited only by proprietary word processors, SGML or XML for which the DTD and/or processing tools are not generally available, and the machine-generated HTML, PostScript or PDF produced by some word processors for output purposes only. The "Title Page" means, for a printed book, the title page itself, plus such following pages as are needed to hold, legibly, the material this License requires to appear in the title page. For works in formats which do not have any title page as such, "Title Page" means the text near the most prominent appearance of the work's title, preceding the beginning of the body of the text. A section "Entitled XYZ" means a named subunit of the Document whose title either is precisely XYZ or contains XYZ in parentheses following text that translates XYZ in another language. (Here XYZ stands for a specific section name mentioned below, such as "Acknowledgements", "Dedications", "Endorsements", or "History".) To "Preserve the Title" of such a section when you modify the Document means that it remains a section "Entitled XYZ" according to this definition. The Document may include Warranty Disclaimers next to the notice which states that this License applies to the Document. These Warranty Disclaimers are considered to be included by reference in this License, but only as regards disclaiming warranties: any other implication that these Warranty Disclaimers may have is void and has no effect on the meaning of this License. 2. VERBATIM COPYING You may copy and distribute the Document in any medium, either commercially or noncommercially, provided that this License, the copyright notices, and the license notice saying this License applies to the Document are reproduced in all copies, and that you add no other conditions whatsoever to those of this License. You may not use technical measures to obstruct or control the reading or further copying of the copies you make or distribute. However, you may accept compensation in exchange for copies. If you distribute a large enough number of copies you must also follow the conditions in section 3. You may also lend copies, under the same conditions stated above, and you may publicly display copies. 3. COPYING IN QUANTITY If you publish printed copies (or copies in media that commonly have printed covers) of the Document, numbering more than 100, and the Document's license notice requires Cover Texts, you must enclose the copies in covers that carry, clearly and legibly, all these Cover Texts: Front-Cover Texts on the front cover, and Back-Cover Texts on the back cover. Both covers must also clearly and legibly identify you as the publisher of these copies. The front cover must present the full title with all words of the title equally prominent and visible. You may add other material on the covers in addition. Copying with changes limited to the covers, as long as they preserve the title of the Document and satisfy these conditions, can be treated as verbatim copying in other respects. If the required texts for either cover are too voluminous to fit legibly, you should put the first ones listed (as many as fit reasonably) on the actual cover, and continue the rest onto adjacent pages. If you publish or distribute Opaque copies of the Document numbering more than 100, you must either include a machine-readable Transparent copy along with each Opaque copy, or state in or with each Opaque copy a computer-network location from which the general network-using public has access to download using public-standard network protocols a complete Transparent copy of the Document, free of added material. If you use the latter option, you must take reasonably prudent steps, when you begin distribution of Opaque copies in quantity, to ensure that this Transparent copy will remain thus accessible at the stated location until at least one year after the last time you distribute an Opaque copy (directly or through your agents or retailers) of that edition to the public. 8 Lizenz 9 It is requested, but not required, that you contact the authors of the Document well before redistributing any large number of copies, to give them a chance to provide you with an updated version of the Document. 4. MODIFICATIONS You may copy and distribute a Modified Version of the Document under the conditions of sections 2 and 3 above, provided that you release the Modified Version under precisely this License, with the Modified Version filling the role of the Document, thus licensing distribution and modification of the Modified Version to whoever possesses a copy of it. In addition, you must do these things in the Modified Version: • A. Use in the Title Page (and on the covers, if any) a title distinct from that of the Document, and from those of previous versions (which should, if there were any, be listed in the History section of the Document). You may use the same title as a previous version if the original publisher of that version gives permission. B. List on the Title Page, as authors, one or more persons or entities responsible for authorship of the modifications in the Modified Version, together with at least five of the principal authors of the Document (all of its principal authors, if it has fewer than five), unless they release you from this requirement. • C. State on the Title page the name of the publisher of the Modified Version, as the publisher. • D. Preserve all the copyright notices of the Document. • E. Add an appropriate copyright notice for your modifications adjacent to the other copyright notices. • F. Include, immediately after the copyright notices, a license notice giving the public permission to use the Modified Version under the terms of this License, in the form shown in the Addendum below. • G. Preserve in that license notice the full lists of Invariant Sections and required Cover Texts given in the Document's license notice. • H. Include an unaltered copy of this License. • I. Preserve the section Entitled "History", Preserve its Title, and add to it an item stating at least the title, year, new authors, and publisher of the Modified Version as given on the Title Page. If there is no section Entitled "History" in the Document, create one stating the title, year, authors, and publisher of the Document as given on its Title Page, then add an item describing the Modified Version as stated in the previous sentence. • J. Preserve the network location, if any, given in the Document for public access to a Transparent copy of the Document, and likewise the network locations given in the Document for previous versions it was based on. These may be placed in the "History" section. You may omit a network location for a work that was published at least four years before the Document itself, or if the original publisher of the version it refers to gives permission. • K. For any section Entitled "Acknowledgements" or "Dedications", Preserve the Title of the section, and preserve in the section all the substance and tone of each of the contributor acknowledgements and/or dedications given therein. • L. Preserve all the Invariant Sections of the Document, unaltered in their text and in their titles. Section numbers or the equivalent are not considered part of the section titles. • M. Delete any section Entitled "Endorsements". Such a section may not be included in the Modified Version. • N. Do not retitle any existing section to be Entitled "Endorsements" or to conflict in title with any Invariant Section. • O. Preserve any Warranty Disclaimers. If the Modified Version includes new front-matter sections or appendices that qualify as Secondary Sections and contain no material copied from the Document, you may at your option designate some or all of these sections as invariant. To do this, add their titles to the list of Invariant Sections in the Modified Version's license notice. These titles must be distinct from any other section titles. You may add a section Entitled "Endorsements", provided it contains nothing but endorsements of your Modified Version by various parties--for example, statements of peer review or that the text has been approved by an organization as the authoritative definition of a standard. You may add a passage of up to five words as a Front-Cover Text, and a passage of up to 25 words as a Back-Cover Text, to the end of the list of Cover Texts in the Modified Version. Only one passage of Front-Cover Text and one of Back-Cover Text may be added by (or through arrangements made by) any one entity. If the Document already includes a cover text for the same cover, previously added by you or by arrangement made by the same entity you are acting on behalf of, you may not add another; but you may replace the old one, on explicit permission from the previous publisher that added the old one. The author(s) and publisher(s) of the Document do not by this License give permission to use their names for publicity for or to assert or imply endorsement of any Modified Version. • 5. COMBINING DOCUMENTS You may combine the Document with other documents released under this License, under the terms defined in section 4 above for modified versions, provided that you include in the combination all of the Invariant Sections of all of the original documents, unmodified, and list them all as Invariant Sections of your combined work in its license notice, and that you preserve all their Warranty Disclaimers. The combined work need only contain one copy of this License, and multiple identical Invariant Sections may be replaced with a single copy. If there are multiple Invariant Sections with the same name but different contents, make the title of each such section unique by adding at the end of it, in parentheses, the name of the original author or publisher of that section if known, or else a unique number. Make the same adjustment to the section titles in the list of Invariant Sections in the license notice of the combined work. In the combination, you must combine any sections Entitled "History" in the various original documents, forming one section Entitled "History"; likewise combine any sections Entitled "Acknowledgements", and any sections Entitled "Dedications". You must delete all sections Entitled "Endorsements". 6. COLLECTIONS OF DOCUMENTS You may make a collection consisting of the Document and other documents released under this License, and replace the individual copies of this License in the various documents with a single copy that is included in the collection, provided that you follow the rules of this License for verbatim copying of each of the documents in all other respects. You may extract a single document from such a collection, and distribute it individually under this License, provided you insert a copy of this License into the extracted document, and follow this License in all other respects regarding verbatim copying of that document. 7. AGGREGATION WITH INDEPENDENT WORKS A compilation of the Document or its derivatives with other separate and independent documents or works, in or on a volume of a storage or distribution medium, is called an "aggregate" if the copyright resulting from the compilation is not used to limit the legal rights of the compilation's users beyond what the individual works permit. When the Document is included in an aggregate, this License does not apply to the other works in the aggregate which are not themselves derivative works of the Document. If the Cover Text requirement of section 3 is applicable to these copies of the Document, then if the Document is less than one half of the entire aggregate, the Document's Cover Texts may be placed on covers that bracket the Document within the aggregate, or the electronic equivalent of covers if the Document is in electronic form. Otherwise they must appear on printed covers that bracket the whole aggregate. 8. TRANSLATION Translation is considered a kind of modification, so you may distribute translations of the Document under the terms of section 4. Replacing Invariant Sections with translations requires special permission from their copyright holders, but you may include translations of some or all Invariant Sections in addition to the original versions of these Invariant Sections. You may include a translation of this License, and all the license notices in the Document, and any Warranty Disclaimers, provided that you also include the original English version of this License and the original versions of those notices and disclaimers. In case of a disagreement between the translation and the original version of this License or a notice or disclaimer, the original version will prevail. If a section in the Document is Entitled "Acknowledgements", "Dedications", or "History", the requirement (section 4) to Preserve its Title (section 1) will typically require changing the actual title. 9. TERMINATION You may not copy, modify, sublicense, or distribute the Document except as expressly provided for under this License. Any other attempt to copy, modify, sublicense or distribute the Document is void, and will automatically terminate your rights under this License. However, parties who have received copies, or rights, from you under this License will not have their licenses terminated so long as such parties remain in full compliance. 10. FUTURE REVISIONS OF THIS LICENSE The Free Software Foundation may publish new, revised versions of the GNU Free Documentation License from time to time. Such new versions will be similar in spirit to the present version, but may differ in detail to address new problems or concerns. See http:/ / www. gnu. org/ copyleft/ . Each version of the License is given a distinguishing version number. If the Document specifies that a particular numbered version of this License "or any later version" applies to it, you have the option of following the terms and conditions either of that specified version or of any later version that has been published (not as a draft) by the Free Software Foundation. If the Document does not specify a version number of this License, you may choose any version ever published (not as a draft) by the Free Software Foundation. ADDENDUM: How to use this License for your documents To use this License in a document you have written, include a copy of the License in the document and put the following copyright and license notices just after the title page: Copyright (c) YEAR YOUR NAME. Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, Version 1.2 or any later version published by the Free Software Foundation; with no Invariant Sections, no Front-Cover Texts, and no Back-Cover Texts. A copy of the license is included in the section entitled "GNU Free Documentation License". If you have Invariant Sections, Front-Cover Texts and Back-Cover Texts, replace the "with...Texts." line with this: with the Invariant Sections being LIST THEIR TITLES, with the Front-Cover Texts being LIST, and with the Back-Cover Texts being LIST. If you have Invariant Sections without Cover Texts, or some other combination of the three, merge those two alternatives to suit the situation. If your document contains nontrivial examples of program code, we recommend releasing these examples in parallel under your choice of free software license, such as the GNU General Public License, to permit their use in free software.