*************y*******,***
Werbung

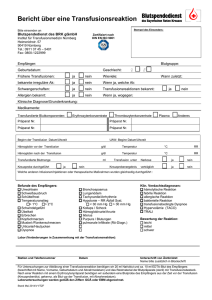
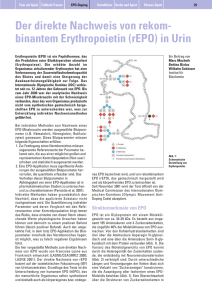
Neues von EPO, Eisen und co. Prof. Dr. T. Frietsch 24.Nov 2012 0 Agenda • Ist Patient Blood Management individuelle Hämotherapie ? • Welche Elemente sind alte Hüte ? • Wie sieht ein Hämotherapeut mit einem alten Hut gut aus ? 1 Patient Blood Management 2 Die Instrumente des PBM Optimierung der Hämatopoese •Anämie: Reduktion des Blutverlusts •Gerinnungsanamnese •Eigenblutspende •Beachte physiologische Reserven •Restriktiver Transfusionstrigger •Minimiere Blutverluste •Sorgfältige Blutstillung •Chirurgische Technik •Hämodilution •Cell Saver •Gerinnungsoptimierung •Optimiere HZV •Optimiere Sauerstoffversorgung •Restriktiver Transfusionstrigger •Achtsamkeit •Monitoring •Aufwärmen •Iatrogene Blutverluste ↓ •Gerinnungstherapie •Stressulkusprophylaxe •Infektionstherapie •Anämietoleranz •Anämietherapie •Sauerstoffverbrauch ↓ •Prompte Infekttherapie Diagnose und Behandlung •Planung Chirurgie •Anämiebehandlung: Eisen Erythropoetin 3 Postoperative Anämie 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Agenda • Ist Patient Blood Management individuelle Hämotherapie ? • Welche Elemente sind alte Hüte ? • Wie sieht ein Hämotherapeut mit einem alten Hut gut aus ? 4 Die autologe Hämotherapie • • • 1. Akute normovolämische Hämodilution 2. Eigenblutspende 3. Cell Saver- Maschinelle Autotransfusion Segal JB, Blasco-Colmeanres E, Norris EJ, Guallar E: Preoperative acute normovolemic hemodilution: a meta-analysis. Transfusion 2004;44:632-644 Carless P, Moxey A, O'Connell D, Henry D. Autologous transfusion techniques: a systematic review of their efficacy. Transfus Med 2004; 14: 123–144. 5 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Die autologe Hämotherapie • • • • 1. Akute normovolämische Hämodilution 2. Eigenblutspende 3. Cell Saver- Maschinelle Autotransfusion 4. Erythropoetin/Eisentherapie Forgie MA, Wells PS, Laupacis A, Fergusson D. Preoperative autologous donation decreases allogeneic transfusion but increases exposure to all red blood cell transfusion: results of a meta-analysis. International Study of Perioperative Transfusion (ISPOT) Investigators. Arch Intern Med. 1998 Mar 23;158(6):610-6 Lorentz A, Osswald PM, Schilling M, Jani L. A comparison of autologous transfusion procedures in hip surgery. Anaesthesist 1991 Apr;40(4):205-13. 6 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Die autologe Hämotherapie • • • • 1. Akute normovolämische Hämodilution 2. Eigenblutspende 3. Cell Saver- Maschinelle Autotransfusion 4. Erythropoetin/Eisentherapie Laupacis A, Fergusson D. Erythropoietin to minimize perioperative blood transfusion: a systematic review of randomized trials. The International Study of Peri-operative Transfusion (ISPOT) Investigators. Transfus Med. 1998 Dec;8(4):309-17. Devon KM, McLeod RS. Pre and peri-operative erythropoietin for reducing allogeneic blood transfusions in colorectal cancer surgery. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD007148. 7 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Die autologe Hämotherapie • • • 1. Akute normovolämische Hämodilution 2. Eigenblutspende 3. Cell Saver- Maschinelle Autotransfusion Waters JH, Yazer M, Chen YF, Kloke J. Blood salvage and cancer surgery: a meta-analysis of available studies. Transfusion 2012; [Epub ahead of print]. 8 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf rHuEPO Therapie (seit 1985) NHS, Dialyse (Besarab et al) CHOIR, Nicht-D (Singh et al) CREATE, Nicht-D (Drüeke et al) TREAT, Nicht-D (Pfeffer et al) Hämatokrit (%) 45 500 E/kg 150 E/kg 40 Thrombose-Inzidenz erhöht Seit 23. 10. 2007 geänderte Empfehlungen der EMA (“European Medicines Agency“) zur Anwendung Erythropoiese stimulierender Agenzien (ESA): 35 Indikation: symptomatische Anämie Behandlungsziel: [Hb] 100 - 120 g/L 30 50 E/kg [Hb] soll 120 g/L nicht überschreiten 25 www.emea.europa.eu/pdfs/human/ press/pus/49618807en.pdf 15 E/kg 20 15 0 2 4 6 8 10 12 Behandlungswochen (3 x pro Woche, IV) 9 12-07-24 OSP- Kolloqium Nach: Eschbach J et al, N Engl J Med 316: 73-8, 1987 14 16 ESA als Anti-Anämika Wolff M, Fandrey J, Hirner A & Jelkmann W. “Perioperative use of recombinant human erythropoietin in patients refusing blood transfusions. Pathophysiological considerations based on 5 cases“ Eur J Haematol 58: 154-9, 1997 10 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf ESA als Anti-Anämika Zeckey C, Vanin N, Neitzke G, Mommsen P, Bachmann S, Frink M, Wilhelmi M, Krettek C, Hildebrand F (MHH). „Zeugen Jehovas und Schwerverletzung mit drohender Hämorrhagie - Wie komplex ist die Behandlung?“ Chirurg 82: 531-5, 2011. 20-jährige Patientin, PKW-Unfall (Glasgow Coma Scale 10) Verlauf von [Hb] und Gerinnungssituation Ab 1. Tag rHuEPO (30.000 E/d/IV f. 5 d), täglich enteral Eisen (600 mg/d), parenteral Vit. B6 (100 mg/d) u. B12 (1000 µg/d). Nach 5 Tagen unauffällige Beatmungspara-meter u. regelrechte Oxygenierung. rHuEPO 30.000 E 11 PPSB (Prothrombinkonzentrat): Prothrombin, Prokonvertin, Stuart-Prower Faktor, antihämophiler Faktor B ESA als Anti-Anämika Nachteile blutgruppenkompatibler Erythrozytentransfusionen Kosten Infektionsrisiko (Bakterien, Hepatitis-, Zytomegalie- und Retroviren) Embolie Hypervolämie +) Critical Elektrolytstörungen (Zitrat, Corwin HL et al for the EPO Care Trials Group. “Efficacy andKsafety of epoetin alfa in critically ill patients”. New Engl J Med 357: 965-76, 2007 Überladung des Organismus mit Eisen (Hämosiderose) Sensibilisierung gegen Histokompatibilitätsantigene Immunsuppression (Tumorrezidivhäufigkeit?) Hypothese: ESA-Therapie vermindert Ery-Transfusionsnotwendigkeit Corwin HL et al for EPO Critical Care Trials Group. “Efficacy and safety of epoetin alfa in critically ill patients”. N Engl J Med 357: 965-76, 2007 12 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf ESA als Anti-Anämika Design: Prospektiv, randomisiert, Plazebo kontrolliert; 1460 innere, chirurg. bzw. Trauma-Patienten, 48-96 h nach Aufnahme auf Intensivstation; 40.000 E rHuEpo wöchentlich, bis zu 3 Wochen. Primärer Endpunkt: Prävalenz von Transfusionen (“Transfusion Trigger” [Hb] >90 g/L); sekundär: Anzahl d. Transfusionen, Mortalität u. [Hb]. Ergebnisse: Transfusion unverändert, [Hb] u. Inzidenz thromboembolischer Ereignisse erhöht, Mortalitätsrate tendenziell vermindert. Kaplan-Meier-Plot, Mortalität, Tag 29, 733 rHuEPO- u. 727 Plazebo-Patienten “62 patients died in the epoetin alfa (8.5%) and 83 in the placebo group (11.4%)….. Kaplan-Meier estimates for trauma patients were similar to those in the figure (P = 0.04).” Corwin HL et al. “Efficacy and safety of epoetin alfa in critically ill patients”. N Engl J Med 357: 965-76, 2007 13 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf ESA als Anti-Anämika Minderung der Transfusionsbedürftigkeit (Meta-Analyse) Zarychanski R et al. “Erythropoietin-receptor agonists in critically ill patients: a meta-analysis of randomized controlled trials“. Can Med Assoc J 177: 725-34, 2007 “Analysis of transfusion independence among critically ill patients“ CI = confidence interval 14 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Kanakaris NK et al, Dept Trauma & Orthopaedics, Leeds, UK. The role of erythropoietin in the acute phase of trauma management: Evidence today Injury 40: 21-27, 2009 Summary “Trauma patients often present in a state of haemorrhagic shock. Blood products remain the gold standard of resuscitation, but allogeneic blood transfusions (ABTs) are associated with several risks. The stimulating effect of recombinant-erythropoietin (EPOA) on erythropoiesis has raised interest in its administration as an alternative. The existing evidence on the early use of EPO-A in the acute phase of trauma patients management consists of only 14 publications. The level of evidence of these studies and the number of treated patients was not found to be adequate to support its generalised use, despite their favourable results. Its safety profile, the preliminary proofs of its efficacy, and the additional cytoprotective properties of EPO-A strongly encourage further controlled studies assessing its use in the acute setting of initial trauma management. …..” Conclusion “…… it has a safe profile at the standard doses of elective cases, and is effective in low energy hip-trauma in the elderly…..“ 15 ESA als Anti-Anämika Corwin HL: “Erythropoietin use in critically ill patients: forest and trees”. Can Med Assoc J 177(7): 747-9, 2007 * * Corwin HL et al, N Engl J Med 357: 965-76, 2007 Internistische und Chirurgische Intensivpatienten, 40.000 E Epoetin alfa/Woche + Eisen f. 3 Wochen 16 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf ESA als Anti-Anämika Minderung der Transfusionsbedürftigkeit (Meta-Analyse) Zarychanski R et al. “Erythropoietin-receptor agonists in critically ill patients: a meta-analysis of randomized controlled trials“. Can Med Assoc J 177: 725-34, 2007 “Analysis of transfusion independence among critically ill patients“ CI = confidence interval 17 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf Agenda • Ist Patient Blood Management individuelle Hämotherapie ? • Welche Elemente sind alte Hüte ? • Wie sieht ein Hämotherapeut mit einem alten Hut gut aus ? 18 Individuelle Hämotherapie 19 Willkommen zur interdisziplinären Regelung Wie berechne ich eigene Produkte? Welche Kombination autologer Verfahren? Eigenblutspende 20 MAT Linzer Transfusionsgespräche 2010 Workshop STrategie/Ökonomie Eigenblutspende Effektivität Author Goodnough et al. 1989+1992 Wittig et al. 1994 Singbartl et al. 2007 Trial Patients (RCT) Most orthop. Surgery RCT orthop. Patients 21/19 BS orthop. Patients 150/84 Donations Additional Result 2 x per week over a 21 day period Data from RCT: EPO vs KG Gained red cell mass 568 ml (aim: 6 units) days 0,3,7 (14) vs. days 0,7,14 (21) (aim: 3 units) Double donation (Apheresis) vs. single 1x Week (aim: 2 units) Gained red cell mass (total preop) 1633 vs 1474 ml p < 0.05 Gained red cell mass : 261 vs 168 ml (A) 238 vs 149 ml (RA) p < 0,000 resp. 0,039 Goodnough et al. Preoperative red cell production in patients undergoing aggressive autologous blood phlebotomy with and without erythropoietin therapy. Transfusion. 1992 Jun;32(5):441-5. Goodnough et al. The effect of patient size and dose of recombinant human erythropoietin therapy on red blood cell volume expansion in autologous blood donors for elective orthopedic operation. J Am Coll Surg. 1994 Aug;179(2):171-6 Wittig et al. Short donation intervals in preoperative autologous blood donation in the concept of autologous transfusion. Anaesthesist. 1994 Jan;43(1):9-15. Singbartl et al. Preoperative autologous blood donation - part II. Adapting the predeposit concept to the physiological basics of erythropoiesis improves its efficacy. Minerva Anestesiol. 2007 Mar;73(3):153-60. HAI Berlin 17.-19.09.09 Linzer Transfusionsgespräche 2010 21 Workshop STrategie/Ökonomie Infektions- und Transfusionsraten ohne Einschränkung Hb-Wert Transfusionen Strategie EPO Strategie Autolog Strategie Allogen Infektionen Strategie EPO 7,0% 9,8% 8,7% 9,7% 21,4% 2,2% Strategie Autolog 2,8% Strategie Allogen 2,8% Transfusion Autolog (%) Autolog und Allogen Transfusion Allogen (%) 22 22 Standard in Studien (Ferritin > 100 μg/l und/oder TSAT > 20%) -4 Monate -3 Monate -2 Monate -1 Monat EP O s.c. ERYPO 40.000 IE s.c. 200 mg Fe-IISubstitution pro Tag OP EP O s.c. EP O s.c. Eisen per os EP O s.c. +Fe p.o. /i.v. Standard bei Eisenmangel (Ferritin < 100 μg/l und/oder TSAT < 20%) -4 Monate ERYPO 40.000 IE s.c. i.v. entsprechend Eisenmangel p.o. 200 mg Fe-IISubstitution pro Tag 23 -3 Monate -2 Monate -1 Monat OP EP O s.c. EP O s.c. EP O s.c. EP O s.c. +Fe i.v. +Fe i.v. +Fe i.v. +Fe i.v. oder Eisen per os +Fe p.o. /i.v. Stratifiziert nach Hb-Wert und dosisadaptiert (Ferritin > 100 μg/l und/oder TSAT > 20%) Ziel 15g/dl präoperativer Hb-Wert 10-12 g/dl -4 Monate -3 Monate -2 Monate ERYPO Nach FachInformation 600 I.E./kg KG zum Bsp.: -1 Monat EPO s.c. 68kg KG = 40 000 I.E. (40K) 85kg KG= 40K + 10K EPO s.c. EPO s.c. Eisen per os -4 Monate -2 Monate 102kg KG= 40K + 20K -1 Monat EPO s.c. 136kg KG= 40K + 40K EPO s.c. EPO s.c. Eisen per os +Fe p.o. /i.v. Ziel 15g/dl präoperativer Hb-Wert 13 g/dl i.v. entsprechend Eisenmangel p.o. 200 mg Fe-IISubstitution 24 pro Tag -4 Monate -3 Monate -2 Monate +Fe p.o. /i.v. OP 119kg KG= 40K + 30K FERRITIN EPO s.c. Ziel 15g/dl präoperativer Hb-Wert 12-13 g/dl -3 Monate OP -1 Monat EPO s.c. OP EPO s.c. Eisen per os +Fe p.o. /i.v. Modell Damp (elektive Orthopädie) ERYPO Nach FachInformation 600 I.E./kg KG zum Bsp.: Diagnostik präoperativer Hb-Wert 10-11 g/dl Eisendiagnostik Ohne path. Befund Ziel 13g/dl Bei isoliertem Fe+ Mangel -3 Wochen -2 Wochen -1 Woche EPO s.c. +Fe i.v. 102kg KG= 40K + 20K 119kg KG= 40K + 30K OP Var. Zusätze 68kg KG = 40 000 I.E. (40K) 85kg KG= 40K + 10K präoperativer Hb-Wert < 10 g/dl OP EPO s.c. EPO s.c. +Fe p.o. /i.v. +Fe i.v. Bei normalem Fe+ -3 Wochen 136kg KG= 40K + 40K -2 Wochen präoperativer Hb-Wert 11-13 g/dl -1 Woche Ziel 14g/dl OP FERRITIN i.v. entsprechend Eisenmangel p.o. 200 mg Fe-IISubstitution 25 pro Tag EPO s.c. EPO s.c. +Fe i.v. Welche Instrumente ? Welche Kombination autologer Verfahren? EPO vs. Eigenblutspende vs. Kostenkalkulationsmodell/Flash-Animation 26 Linzer Transfusionsgespräche 2010 Workshop STrategie/Ökonomie MAT Fazit Therapeut ? 27 12-11-24 5. DRK Hämotherapie-Symposium: Perioperative fremdblutsparende Verfahren - Bad Sassendorf