G-CSF und ESF in der Hämatologie und Onkologie
Werbung

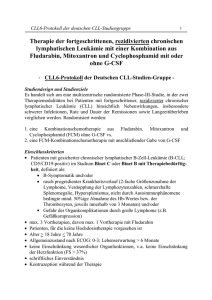
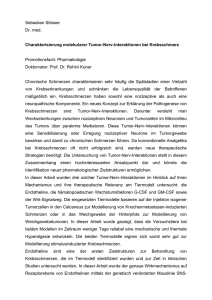
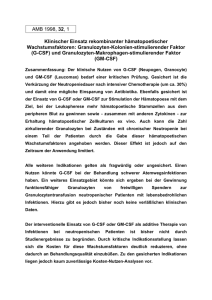
G-CSF und ESF in der Hämatologie und Onkologie T. Kegel, Berlin, 10.01.2006 Martin-Luther-Universität Halle-Wittenberg Klinik für Innere Medizin IV, Hämatologie/ Onkologie Ernst-Grube-Str. 40 06120 Halle Klinische Vorteile der Pegylierung von Proteinen • Verbesserte Pharmakokinetik – längere Serumhalbwertszeit – bessere Wasserlöslichkeit und bessere Bioverfügbarkeit • Konstantere Plasmaspiegel • Höhere biologische Aktivität • Reduktion der Toxizität • geringere Immunogenität Die Pegylierung verändert nicht die biologische Wirkung von Filgrastim in vitro (Proliferationsassay, Rezeptorbindung, Neutrophilenbildung und -funktion ) Luxon et al. From Research to Practice 2001;3 (1): 3-9 Pharmakokinetik von Filgrastim und Pegfilgrastim bei gesunden Probanden Mittlere Zytokinkonz. Im Serum (ng/mL) 100 Pegfilgrastim, 60µg/kg (n=9) Filgrastim, 5µg/kg (n=8) 10 1 0.1 0.01 0 2 4 6 8 Tag 10 12 14 Pegfilgrastim verbleibt im Plasma bis sich die Neutrophilenzahl normalisiert 1,000 Pegfilgrastim 100 µg/kg ANZ 100 100 10 1 1 9 10 ANZ (x 10 /l) Pegfilgrastim-Serumkonzentration (ng/ml) 1,000 0.1 0.1 0.01 0.01 0 3 6 9 12 15 18 21 Zyklus 1 (Tage) ANZ = absolute Neutrophilenzahl Holmes F, et al. J Clin Oncol. 2002;20:727-731. Pegfilgrastim – Abbau durch Neutrophilenvermittelte Selbstregulation Modell der Rezeptor-vermittelten Endozytose von Pegfilgrastim Kotte-Komo AC et al. Pharmacological Research. 2004;50:55-58. National Comprehensive Cancer Network (NCCN) – Clinical Practice Guidelines in Oncology – v.2.2005 National Comprehensive Cancer Network (NCCN) – Clinical Practice Guidelines in Oncology – v.2.2005 Treatment intention Primary G-CSF Prophylaxis in Chemotherapy High (> 20%) • TAC • Topotecan • Docetaxel qw3 Risk of febrile neutropenia Intermediate (10-20%) • AC • Doc/Cape • R-CHOP • Irinotecan/Gem Low (< 10%) • Capecitabine mono • FOLFOX Curative/Adjuvant Prolong survival/ Quality of life G-CSF G-CSF (LOE I) (LOE I) Symptom management/ Quality of life G-CSF Individuelle Entscheidung (Risikofaktoren u.a. Alter>65 Jahre, Vor-Chemotherapie, Herz-und Leberfunktion) Consider G-CSF Risikofaktoren No G-CSF Consider G-CSF Consider G-CSF Risikofaktoren No G-CSF Risikofaktoren No G-CSF National Comprehensive Cancer Network (NCCN) – Clinical Practice Guidelines in Oncology – v.2.2005 Percent FN (%) Neutropenia and Risk of Febrile Neutropenia 50 39% 40 30 19% 20 10 11% 0% 3% 0 0 1 2 3 >=4 Duration of Severe Neutropenia (Days) B odey G P et al. A nn Intern M ed. 1966;64:328-340; M eza L et al. Proc A m Soc C lin O nc ol. 2002;21:255b.A bstra ct 2840. 6 4.0 3.3 4 3.2 2.9 2.3 3 2.3 2.1 2.0 1.6 2 1.6 1.5 1.4 1.3 1 Se ps is D C is er ea eb se ro va sc R ul en ar al D is ea Li ve se rD is ea se Pn G eu ra m m on +v ia e Se ps Pu H y is lm po on te ns ar y Em ion bo lis m Le uk ae H ea m ia rt D is H ea yp se ov Fu ol C on ae ng m ge al ia st I n iv fe e ct H io ea n rt Fa ilu re 0 Lu ng ra m G 4.8 5 –v e Odds Ratios [95% CIs] for Age-Adjusted Mortality Mortality During Hospitalisation for Established FN: Multivariate Logistic Regression Analysis CI = confidence interval; –ve = negative; +ve = positive Kuderer N, et al. Proc Am Soc Clin Oncol. 2004;22.Abstract 6049. Meta-analysis of prophylactic G-CSF in cancer patients receiving chemotherapy • Metaanalyse aus 14 Randomisierten Studien • N=3091 Patienten (Kontrolle: 1544; G-CSF: 1547) • Entitäten: Lymphome, Solide Tumoren (N=8) Results: FN N FN gesamt P-value 892 FN Kontr 576 (37%) FN G-CSF 316 (20,4%) Sub grup pen Ana Lyse RR IRM 10 trials IRM ges N RR P-value 0,55 0,05 2483 IRM Kontr 55 (4,4%) 30 (2,4%) 0,54 <0,001 IRM G-CSF Lymphome 0,69 <0.001 Lymphome 0,58 0,068 Solide Npl 0,45 <0.001 Solide Npl 0,47 0,032 Elderly 0,69 <0.001 Elderly 0,51 0,045 Placebokontr. 0,49 <0.001 Filgrastim 0,58 <0.001 Filgrastim 0,51 0,006 Lenograstim 0,78 0,032 Lenograstim 1,00 0,997 PEGFilgrastim 0,08 <0,001 PEGFilgrastim 0,26 0,30 Dosisintensität (8 trials, N= 1574 pts.): Kontr.: 88,1% vs. G-CSF: 94,5% • Schlussfolgerungen: • G-CSF Prophylaxe reduziert FN-Inzidenz (signifikant) und IRM • Die Dosisintensität wird gesteigert Kuderer NM et al.; #8117, ASCO 2005 Delivery of Chemotherapy Planned Dose on Time Improves Outcomes in Adjuvant Breast Cancer Chemotherapy The Milan Study: relapse-free and overall survival with CMF: 20-year follow-up (n = 386) % of planned dose ≥ 85 (n = 42) 1.0 65–84 (n = 94) < 65 (n = 71) 0.8 Control (n = 179) 0.8 Probability of overall survival Probability of relapse-free survival 1.0 0.6 0.4 0.6 0.4 0.2 0.2 0 0 0 5 10 15 Bonadonna G, et al. N Engl J Med. 1995;332:901-906. 0 20 Years after mastectomy 5 10 15 20 Dosisintensivierte Therapie - Rationale Problematik der Chemotherapie • • Resistenzentwicklung Gompertzianische Wachstumskinetik • Pseodoexponentielles Tumorwachstum bis ca 70% der maximalen Tumormasse erreicht sind → Übergang in „steady state“. Die Verdopplungszeit wird mit zunehmender Tumorgrösse immer länger (abnehmender Anteil proliferierender Zellen, zunehmender Zellverlust durch Absterben) d.h. die Aggressivität und Proliferationsgeschwindigkeit des Tumors nehmen mit der Reduktion der Tumorzellmenge zu. • • Norton-Simon-Hypothese („kinetische Resistenz von Tumorzellen“; z. B. G0- Phase) Dosisintensivierung - Rolle der Dosisintensität Dosisintensität = Zytostatika-Dosis/Zeit Standard-Dosis höher dosierte Therapie dosisdichte Therapie Tumor-Zellzahl 1012 1010 10 8 10 6 10 4 10 2 0 0 8 16 24 0 8 16 24 0 8 16 24 Zeit (Wochen) Eine definierte Dosis eines Zytostatikums tötet eine konstante Tumorzellfraktion, unabhängig von der jeweils vorhandenen Tumorzellmasse, solange das Wachstum konstant exponentiell erfolgt nach Norton, 1997; „Zelltodhypothese“ n. Skipper, Schabel und Wilcox, 1964 AGO-ETC – Studiendesign (N=1144 Pat.) Epirubicin 150 mg/m² q2w x 3 Paclitaxel 225 mg/m² q2w x 3 Cyclophosphamide 2500 mg/m² q2w x 3 + TAM R R G-CSF (Neupogen) ± Epoetin-α EC 90/600 mg/m² ( ) Paclitaxel 175 mg/m² + TAM q3w x 4 Möbus et al, Proc ASCO 2004; 23: # 513 q3w x 4 AGO-ETC - Hämatologische Toxizität EC → T ETC NCI-Grad 0 1 2 3 4 7% 1% 9% 11% 24% 46% 4% 10% 38% 44% 4% =.0009 2% 95% 3% <.0001 Anämie 16% 26% 49% Leukopenie 10% Thrombopenie 57% 20% 14% Febrile Neutropenie 7% Möbus et al, Proc ASCO 2004; 23: # 513 7% 0 1 2 45% 36% 18% 1% 2% 3 p-Wert 1% 4 0% 1% 0% <.0001 <.0001 AGO-ETC - Zeit bis zum Rezidiv, 28 Monate f/u 1.0 Progressionsfrei 0.8 0.6 0.4 0.2 ETC n = 590, 94 Ereignisse EC -> T n = 554, 127 Ereignisse p = 0.0009 0.0 0 12 24 36 Monate Möbus et al, Proc ASCO 2004; 23: # 513 48 60 AGO-ETC - OS nach median 28 Monaten f/u Gesamtüberleben 1.0 0.8 0.6 0.4 ETC 0.2 n = 590, 43 Ereignisse EC -> T n = 554, 60 Ereignisse p = 0.030 0.0 0 12 24 36 Monate Möbus et al, Proc ASCO 2004; 23: # 513 48 60 CHOP-14 Improves Survival Compared with CHOP-21 in Patients (> 60 Years) with NHL Proportion Surviving 1.0 RR death CHOP-14 vs CHOP-21: 0.58 (0.43–0.79; P < 0.001) 0.8 69% 0.6 53% CHOP-14 (n = 172) CHOEP-14 (n = 169) CHOEP-21 (n = 170) CHOP-21 (n = 178) 0.4 0.2 0 0 10 20 49% 41% 5 years 3 years 30 40 50 Months 60 70 80 90 G-CSF was administered with CHOP-14 CHOP = cyclophosphamide, doxorubicin, vincristine, prednisone; CHOEP = CHOP + etoposide; NHL = non-Hodgkin’s lymphoma; RR = relative risk Pfreundschuh M, et al. Blood. 2004;104:634-641. Cumulative Risk of FN by Age NHL: CHOP (n = 577) 0.40 ≥ 65 years Cumulative Risk of FN Cycle 1 0.30 P = 0.0002 0.20 < 65 years 0.10 0 0 20 40 60 80 100 Days to First FN Episode CHOP = cyclophosphamide, doxorubicin, vincristine, prednisone 120 140 Lyman GH, et al. Leuk Lymphoma. 2003;44:2069-2076. Fallvorstellung 1: Patient, 28-jährig, Reizhusten, Nachtschweiss, Gewichtsverlust • 12/2003 Reizhusten, Nachtschweiss, Gewichtsverlust >10% in 3 Monaten, Schwellung Supraclavikulargrube rechts, Splenomegalie. Röntgen/CT-Thorax: Mediastinale Lymphknotenvergrösserung mit beginnender Kompression der V. cava superior. • 01/2004 CT-gestützte Lymphknotenbiopsie mediastinal. Histologie: Hodgkin Lymphom vom Typ der nodulären Sklerose. • Ausbreitungsdiagnostik (CT-Abdomen, PET, Labor): CS III BS + RF a, b (Extranodalbefall: Milz). • Spermakryokonservierung. • 01/2004 Randomisation in HD 15, Arm B ⇒ 6# BEACOPP eskaliert. Fallvorstellung 1: Patient, 28-jährig, M. Hodgkin CS IIIBS • 01-05/04 6 # BEACOPP eskaliert. Therapieprotokoll „BEACOPP eskaliert“ Cyclophosphamid i.v. Tag 1 Neutropenie 35 mg/m² i.v. Tag 1 Thrombozytopenie Etoposid 200 mg/m² i.v. Tag 1-3 Procarbazin 100 mg/m² p.o. Tag 1-7 40 mg/m² p.o. Tag 1-14 Prednison Vincristin 1,4 mg/m² (max.2mg) i.v. Tag 8 Bleomycin 10 mg/m² i.v. Tag 8 s.c. Ab Tag 8 G-CSF • Hämatotoxizität 1250 mg/m² Adriamycin • ( Wdh. Tag 22) Febrile Neutropenie Grad 2 Grad 3 Grad 4 Zyklus 1-3 Zyklen 4-6 Zyklen 1-6 - Therapiebeurteilung (Abschlusstaging) 05/04: Partialremission mit residualen mediastinalen Lymphknoten bis 23 mm. PET negativ. Keine Bestrahlung. Nachsorge 12/05: Vollständige Regredienz der Lymphknoten. Kein Rezidiv! Clinical Benefit of Pegfilgrastim at 40% Risk of FN FN Rate (%) Registration pegfilgrastim studies Clinical benefit in myelosuppressive chemotherapy Expected FN incidence ~ 40%* 40 (n = 42) 35 38 Expected Filgrastim Pegfilgrastim 30 25 (n = 80) 20 20 15 (n = 77) 10 18 (n = 154) 13 5 0 (n = 156) Misset et al.1 Green et al.2 9 Holmes et al.3 1Misset mg/m2 *Doxorubicin 60 Q3W and docetaxel 75 mg/m2 Q3W JL, et al. Ann Oncol. 1999;10:553-560; 2Green MD, et al. Ann Oncol. 2003;14:29-35; 3Holmes FA, et al. J Clin Oncol. 2002;20:727-731. FN-Related Hospitalisation (%) 20 17 15 P < 0.0001 10 5 0 1 Placebo IV = intravenous 16 14 12 P < 0.0001 8 4 1 0 Placebo Pegfilgrastim Use of FN-Related IV Anti-Infective (%) Incidence of FN (%) Pegfilgrastim Virtually Eliminated FN in Patients Receiving Moderately Myelotoxic Chemotherapy (at 20% Risk of FN) 12 10 Pegfilgrastim 10 8 P < 0.0001 6 4 2 2 0 Placebo Pegfilgrastim Schwartzberg LS, et al. Support Care Cancer. 2004;12:382. Abstract A-52 Der Einsatz von G-CSF und ESF in der onkologischen Palliativtherapie Palliative Chemotherapie QoL Überlebensvorteil Remissionsdruck Infektionen Knochenmarkinsuffizienz Schmerzreduktion Dosisintensivierte CTX Einflussstauung Vital bedrohlichtoxisch toxisch Hospitalisierung Zeitgerechte Therapiefortsetzung Maligner Perikard-/ Pleuraerguss Therapie limitierend Fremdzellinfiltration/ Knochenmarkkarzinose Infektion Beherrschung Onkologische Notfallsituationen Hohe Tumorlast Kontrolle Paraneoplastische Syndrome MDS How does Neutropenia influence quality of life? In a prospective study of patients receiving docetaxel for multiple tumor types (n=25), a greater decline in ANC predicted worse QOL† at nadir for*: – physical functioning (P<0.001) – social functioning (P<0.04) – general physical symptoms (P<0.04) – distress (P<0.04) QOL impairments persist even after neutropenic recovery. As measured by the SF-36, CCM, and Psychosocial Adjustment to Illness Scale. *. Fortner BV, et al. Proc Am Soc Clin Oncol. 2002;21:247b. Abstract 2808. Der Einsatz von G-CSF und ESF in der onkologischen Palliativtherapie Palliative Chemotherapie QoL Überlebensvorteil Remissionsdruck Infektionen Knochenmarkinsuffizienz Schmerzreduktion Dosisintensivierte CTX Einflussstauung Vital bedrohlichtoxisch toxisch Hospitalisierung Zeitgerechte Therapiefortsetzung Maligner Perikard-/ Pleuraerguss Therapie limitierend Fremdzellinfiltration/ Knochenmarkkarzinose Infektion Beherrschung Onkologische Notfallsituationen Hohe Tumorlast Kontrolle Paraneoplastische Syndrome MDS Metastasierendes Mammakarzinom – OR als Surrogatendpunkt für Gesamtüberleben • Metaanalyse: • 10 randomisierte Studien: Standarddosis vs Dosisintensivierter Epirubicinhaltiger Ctx. • N=2.126 Pooled Odds Ratio (95% CI) Response Rate P 0.6 (0.51-0.72) (pooled odds ratio for non-response) OS Response as predictor of OS 0.94 (0.86-1.04) 0.22 < 0.0001 Bruzzi, P. et al. J Clin Oncol; 23:5117-5125 2005 G-CSF in palliative Chemotherapy – Survival • Überlebensvorteil - auch in palliativer Situation - durch geeignete Therapien: – Neue Substanzen/ Kombinationen – Dosiseinhaltung, dosisdichte Therapie, HD Ctx. • Ein direkterer Bezug zum Überleben besteht für lebensbedrohliche onkologischen Notfallsituationen, in denen die weitere Prognose unmittelbar entschieden wird. • Remissionsdruck, Infektionen und KM-Infiltration erfordern die dringliche Einleitung wirksamer Therapien, die häufig nur mit maximalem supportivem Einsatz (u.a. GCSF!) durchführbar sind. Fallvorstellung 2: G-CSF bei onkologischer Notfallsituation • 31-jähriger Patient • 12/92 Tumornephrektomie links. Histologie: Maligner neuroepithelialer Tumor der linken Niere. • 11/00 1. Rezidiv linke Nierenloge → Rezidivoperation als R2-Resektion. Nachfolgend „Immun-/Chemotherapie (FU/IL-2/IFN-G)“ • 08/01 2. Rezidiv/Progress linke Nierenloge sowie Bauchdeckenmetastase → erneut Rezidivoperation, anschliessend aggressive Polychemotherapie nach EURO EWING Protokoll (+Stammzellmobilisierung) + Strahlentherapie ad 50,4 Gy ⇒ PR • 02/02 Progress linke Nierenloge. 2 sequenzielle HD Ctx-Zyklen + PBSCT • 07/02 Residualtumorresektion retroperitoneal: avitales Nekrosengewebe • 11/03 3. Rezidiv im kleinen Becken. Erneute Resektion mit Blasenhinterwandresektion, Ureterreimplantation. • 12/03 Chemotherapie n. Standard P-ICE + G-CSF + S-CF. • 09/04 Progress im kleinen Becken. Notfallaufnahme im Blutungsschock bei massiver Makrohämaturie (Hb 2,9 mmol/l)... Fallvorstellung 2: G-CSF bei onkologischer Notfallsituation Fallvorstellung 2: G-CSF bei onkologischer Notfallsituation • 31-jähriger Patient – Verlauf • Kreislaufstabilisierung und Polytransfusion. • Sofortige urologische Versorgung mittels Zystoskopie und Anlage eines Spülkatheters. Perkutane Nierenfistelung bei Harnaufstau in der Einzelniere rechts. Bei großflächigem Tumoreinbruch in die Harnblase keine Möglichkeit der zystoskopischen/operativen Blutungsstillung. • Notfallmäßige Einleitung einer erneuten perkutanen Strahlentherapie in hämatostyptischer Indikation. Hämatotoxizität: Leukozytopenie Grad 4, Thrombozytopenie Grad 3. Urosepsis!!! • Unter Breitbandantimikrobieller Therapie + G-CSF nach 5 Tagen Leukozytenregeneration und Kontrolle der Sepsis. • Zunächst klinische Restitution, keine weitere Hämaturie. Nachfolgend palliative ambulante Chemotherapie mit Capecitabin + EGF-R Antikörper. Exitus letalis 03/05 bei Progress. Der Einsatz von G-CSF und ESF in der onkologischen Palliativtherapie Palliative Chemotherapie QoL Überlebensvorteil Remissionsdruck Infektionen Knochenmarkinsuffizienz Schmerzreduktion Dosisintensivierte CTX Einflussstauung Vital bedrohlichtoxisch toxisch Hospitalisierung Zeitgerechte Therapiefortsetzung Maligner Perikard-/ Pleuraerguss Therapie limitierend Fremdzellinfiltration/ Knochenmarkkarzinose Infektion Beherrschung Onkologische Notfallsituationen Hohe Tumorlast Kontrolle Paraneoplastische Syndrome MDS Fallbeispiel 3: Remissionsdruck bei Pleuraerguss und oberer Einflussstauung; 24-jähriger Patient mit Rezidiv eines Synovialsarkoms Fallbeispiel 4: Remissionsdruck bei hoher Tumorlast bei Metastasenleber Der Einsatz von G-CSF und ESF in der onkologischen Palliativtherapie Palliative Chemotherapie QoL Überlebensvorteil Remissionsdruck Infektionen Knochenmarkinsuffizienz Schmerzreduktion Dosisintensivierte CTX Einflussstauung Vital bedrohlichtoxisch toxisch Hospitalisierung Zeitgerechte Therapiefortsetzung Maligner Perikard-/ Pleuraerguss Therapie limitierend Fremdzellinfiltration/ Knochenmarkkarzinose Infektion Beherrschung Onkologische Notfallsituationen Hohe Tumorlast Kontrolle Paraneoplastische Syndrome MDS G-CSF bei onkologischer Notfallsituation – Fallbeispiel 5 • 68-jährige Patientin • 05/2003 ED Follikuläres SD-Karzinom mit primärer ossärer Metastasierung. • 05/2003 Fixateur interne BWK 7 – BWK 9 bei instabiler BWS durch Metastasierung bei unbekanntem PT. Histologie: Metastase eines Follikulären SD-Karzinoms. • 06/2003 Thyreoidektomie mit cervikaler Lymphadenektomie und Autotransplantation von Epithelkörperchen. • 09 und 12/2003 Zweimalige Radiojotherapie mit je 6,5 GBq 131-J. • 09.01.2004 Notfallmäßige stationäre Aufnahme über die ZNA der Uni Kliniken: • Somnolente hochfebrile Patientin. RR 85/50 mm Hg. Exsikkose. Hämorrhagische Stomatitis Grad 4. Petechiale und flächenhafte Hauteinblutungen. G-CSF bei onkologischer Notfallsituation – Fallbeispiel 5 • 68-jährige Patientin • Labor (SI-Werte) bei Aufnahme: Hb: 3,0; Hct: 0,14; Leuko: 0,8; Plt 2; CRP 198,9. • Notfalltherapie: Hydrierung, O2-Gabe, Transfusion von Erythrozyten und Thrombozyten, iv-antimikrobielle Breitbandtherapie, tgl. Gabe von G-CSF und Folsäure. Passagere parenterale Ernährung. • Verlauf: • unter o.g. Massnahmen rasche Besserung des AZ. Infektionssituation schnell kontrolliert. CRP fallend. Am 6. stationären Tag Leuko > 1. Prolongierte substitutionspflichtige Thrombozytopenie. Fallbeispiel 6: Aspergillenpneumonie bei 56-jähriger Patientin mit Ph+ ALL Fallbeispiel 5: Deutliche Besserung der Aspergillenpneumonie unter Antimykotika und G-CSF bei 56-jähriger Patientin mit Ph+ ALL Fallbeispiel 6: Infektionen 3: ARDS bei neutropener Sepsis nach Chemotherapie wegen NSCLC u. bei vorbestehendem MDS Der Einsatz von G-CSF und ESF in der onkologischen Palliativtherapie Palliative Chemotherapie QoL Überlebensvorteil Remissionsdruck Infektionen Knochenmarkinsuffizienz Schmerzreduktion Dosisintensivierte CTX Einflussstauung Vital bedrohlichtoxisch toxisch Hospitalisierung Zeitgerechte Therapiefortsetzung Maligner Perikard-/ Pleuraerguss Therapie limitierend Fremdzellinfiltration/ Knochenmarkkarzinose Infektion Beherrschung Onkologische Notfallsituationen Hohe Tumorlast Kontrolle Paraneoplastische Syndrome MDS G-CSF in palliativer Indikation: Patientin mit Knochenmarkkarzinose bei Mammakarzinom Klinisch bewährte Indikationen für G-CSF – Standard an der MLU Halle Neutropenie < 1,0 Gpt/l nach Chemotherapie u./o. Strahlentherapie + stark vorbehandelte Patienten (eingeschränkte Knochenmarkreserve) ++ großvolumige KM-Vorbestrahlung (z. B. Becken) + high grade NHL, CLL mit Ak-Mangel + Neutropenie bei • Alter > 60 J., • hoher Komorbidität + + Jede Infektion bei Neutropenie ++ Infektion mit inadäquatem Leukozytencount + Infektion bei klinisch manifester Immunsuppression ++ Hypoplastisches MDS mit Leukozytopenie - Infektion b. Leukozytopenie bei Hypoplastischem MDS ++ Leukozytopenie nach sequenzieller Radionuklidtherapie + Agranulozytose (medikamentös-allergisch/-toxisch) ++ Erhaltungstherapie bei anhaltender Myelosuppression (toxisch, nach Tx...) + Differenzialindikation für Filgrastim und Pegfilgrastim – wann? was? Therapiesituation Filgrastim Pegfilgrastim Jede Aplasieerzeugende Chemotherapie + + Zyklusdauer < 14 Tage + + Zyklusdauer ≥ 14 Tage + + Patienten Compliance hoch + ++ Patienten Compliance erschwert + +++ Nur seltenerer Arztkontakt + +++ Geplante Stammzellmobilisierung + + Agranulozytose (medikamentös-allergisch/toxisch) ++ ++ Erhaltungstherapie bei anhaltender Myelosuppression (toxisch, n. Tx, ...) + + Leukozytopenie nach sequenzieller Radionuklidtherapie + (+) Nach HD-CTX mit Stammzellrückgabe + ++! Zytokin-abhängige Nebenwirkungen Skelettschmerzen Myalgie Arthralgie Kopfschmerzen ISR Rückenschmerzen Filgrastim n = 151 Pegfilgrastim n = 150 26% 10% 5% 5% 3% 7% 25% 11% 9% 6% 5% 5% National Comprehensive Cancer Network (NCCN) – Clinical Practice Guidelines in Oncology – v.2.2005 New NCCN guidelines In May 2005, the US NCCN launched new guidelines – ‘Myeloid Growth Factors in Cancer Treatment’ – (http://www.nccn.org) These guidelines recommend that – Prophylactic G-CSF should be given to all patients with a >20% risk of FN and considered for those with a 10–20% risk – Patient risk factors should be considered to determine the overall risk of FN – An individual patient’s risk for FN should be re-evaluated every cycle NCCN, National Comprehensive Cancer Network, http://www.nccn.org NCCN, 2005 EORTC G-CSF guidelines: progress Final recommendations likely to complement NCCN Group already considering 20% risk level as the standard for G- CSF intervention Final meeting of the group in September 2005 Guidelines to be submitted as manuscript to EJC in January 2006 Mögliche Auswirkung entsprechender Empfehlungen auf die klinische Praxis • Sorgfältigere Bewertung des FN-Risikos sowie patientenbezogener Risikofaktoren. • Regelmässige Reevaluierung der Risiken (ideal: vor jedem Zyklus). • Reduktion des FN-Risikos durch gezielteren Einsatz von G-CSF. • Reduktion FN-bedingter Komplikationen: Infektionen!, Mortalität, Hospitalisierung, Einschränkung der Lebensqualität, Verbrauch von iv-Antibiotika. • Konsequente Einhaltung der geplanten Dosisintensität → Verbesserte Therapiewirksamkeit. European Guidelines for Anaemia Treatment: Summary • EORTC-endorsed European guidelines for the management of anaemic patients with cancer: – Recommend initiation of ESP therapy at a Hb concentration of 9–11 g/dL, based on anaemia-related symptoms – Recommend a target Hb concentration of 12–13 g/dL • The two major goals of ESP therapy should be to improve QOL and to prevent RBC transfusions • Less frequent administration schedules offer patient benefits – Increased convenience with fewer injections and, possibly, fewer clinic visits – The possibility of administering ESP therapy on the same dosing schedule as chemotherapy Gesicherte und potentielle Palliativindikationen für ESF - Standard an der MLU Halle Palliativsituation Indikation für ESF Hohe Transfusionsfrequenz ++ Antierythrozytäre Antikörper durch Sensibilisierung nach Polytransfusion ++ Prophylaxe der vorgenannten Situation ++ Tumorfatiguesymptomatik + Chemotherapieinduzierte Anämie + Symptomatische Tumoranämie ++ MDS +++ Anämie bei Multiplem Myelom ++ Anämie bei chronischen hämatologischen/ lymphatischen Systemerkrankungen ++ Anämie bei Myeloproliferativem Syndrom -/? Anämie nach sequenzieller Radionuklidtherapie ++ Kontraindikationen gegen Transfusion („Zeugen Jehovas“ etc.) +++