Das Hennebert-Zeichen
Werbung

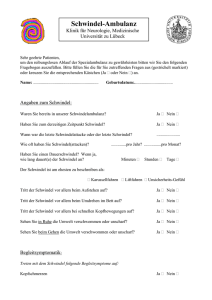
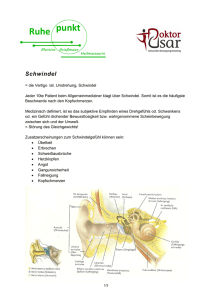
Fistelsymptom, Hennebert-Zeichen, Tulliophänomen und Dehiszenz des vertikalen Bogengangs R. Häusler Universitätsklinik für HNO, Kopf- und Halschirurgie Inselspital Bern Das Fistelsymptom Schwindel und Nystagmus während einer Druckausübung auf den äusseren Gehörgang bei chronischer Otitis mit Trommelfellperforation Æ klassisches Alarmsymptom das aufzeigt, dass ein fortgeschrittenes Cholesteatom zu einer Arrosion des lateralen Bogengangs geführt hat Das Fistelsymptom bei fortgeschrittenem Cholesteatom mit Arrosion des lateralen Bogengangs p Signe classique de la fistule patient atteint d‘un cholestéatome étendude l‘oreille g avec érosion du canal semicirculaire horizontal Das Hennebert-Zeichen (1911) = Schwindel und Nystagmus während einer Druckausübung auf den äusseren Gehörgang bei intaktem Trommelfell Æ galt initial als pathognomonisch für die kongenitale Syphilis Æ ist ein typisches Zeichen für das Vorhandensein eines Innenohrhydrops (Meniere, Syphilis, …) Das Hennebert-Zeichen Signe de Hennebert Maladie de Menière OG Pathophysiologie des Hennebert Zeichens normal M. Meniere (Hydrops des Sacculus bis an Fussplatte Das Tulliophänomen (1919) Schwindel und Nystagmus bei lauter Schalleinwirkung I. Bei Labyrinthfistel Æ initial beschrieben nach experimenteller Bogengangsfistel bei Vögeln (Weltausstellung in Paris, 1928) II. Bei hypermobilem Steigbügel Æ Trompetenspieler Æ Jogger Æ Holzhacker Tullio und Hennebert Brandt, 1998 Tullio-Phänomenon Typ II Hypermobiler Steigbügel Vertigo due toTullio phenomenon and Hennebert sign related to stapeshypermobility can easily be treated by minor otological procedures • Stapes consolidation with or without section of the stapedial tendon • Stapedotomy with a short piston A new neuro-otological Entity: The dehiscence of the vertical semicircular canal first description by Minor et al. Arch Otolaryngol Head and Neck Surg 124, 1998 Pathophysiology third window in the bony labyrinth (two windows good, three windows bad) Normal situation: 2 cochlear windows middle fossa o.w. r.w. i.a.c. Vertical Semicircular canal ical situation: 2 cochlear windows Pathological situation: 2 cochlear windows + 1 additional window in the superior semicircular canal Vestibular Symptoms • Vertigo during pressure changes fistula sign Hennebert sign • Vertigo during acoustic stimulation Tullio phenomenon • Vertigo during Valsalva maneuvre • Oscillopsia Auditory Symptoms • Conductive HL - mainly low frequencies - negative Rinné - stapedial reflexes preserved (DD: otosclerosis !) • Autophonia The audiological and vestibular symptoms may be incomplete and variable The vertical canal dehiscence syndrome: A great otologic mimicker Zhou, Gopen, Poe., Otol Neurootol 28,2007 J.-M. R.,1957 Negative Rinne on both sides Normal tympanic membranes right left Case report III M.K., born 1967, MD • For several months disturbing autophonia in the left ear • Vertigo and nausea when hearing loud noises with the left ear • Vertiginous sensations when applying pressure to the left ear • Vertigo during the Valsalva maneuvre left right Surgical treatment 30.01.2004 • Transtemporal approach • Elevation of the dura from the upper surface of the temporal bone • Identification of the dehiscent vertical semi-circular canal • Sealing of the dehiscence by BoneSource® mixed wich bone pathé Dehiscent superior vertical semi-circular canal Superior petrosal sinus Temporal lobe dura Eminentia arcuata with dehiscent vertical semi-circular canal Post-operative follow-up Immediate relief from: - vertiginous symptoms - Tullio - Hennebert - autophonia M.K.,1967 Post-op Conclusions • The dehiscence of the vertical semi- circular canal is a newly dicovered neurootological entity • The pathophysiological explanation is a supplementary window in the vertical semi-circular canal • Surgical treatment by covering the dehiscence stops the symptoms a The Stockhorn Mountain near Berne in summer (a) and winter (b) as well as superior semicircular canal dehiscence before (c) and after (d) covering with hydroxyapatite cement by a transtemporal approach under computer-assisted navigation. Hearing (pre- (e) and postoperatively (f)) remained normal and Tullio vertigo disappeared postoperatively. b Have a happy c coronal d Pure tone audiogram Pure tone audiogram preoperative right / left postoperative right f e uncovered and rewarding coronal covered New Year ! from Rudolf Häusler Director Department of ENT, Head and Neck Surgery, Inselspital, University of Berne Switzerland Zusätzlich „drittes Fenster“ des superioren Bogenganges Pat. 1 Tullio Oszilopsie Hörminderung Autophonie Tinntius Hennebert Valsalva Schwindel Pat. 2 Pat. 3 Pat. 4 Pat. 5 Pat. 6 Pat. 7 Pat. 8 Pat. 1 Tullio Oszilopsie Hörminderung Autophonie Tinntius Hennebert Valsalva Schwindel Pat. 2 Pat. 3 Pat. 4 Case report I: Z. M., male, 50 years • Hearing loss left ear since several years • Several ear infections • Tympanic membrane with postero-superior retraction pocket • Positive fistula symptom with vertigo Æ Cholesteatoma with semicircular canal arrosion Vertigo due to superior semi-circular canal dehiscence Case report II: J.-M. R.,1957 • Bilateral conductive hearing loss with negative Rinne • Patient referred for stapedotomy Case report II J.M.R., 1957 For several years bilateral hearing loss + vertigo - when hearing loud sounds - when putting pressure on his ears - during airplane trips Case report II J.M. R., 1957 • Bilatera conductive hearing loss in the low frequency range • Stapedial reflex present • Tullio with vertical nystagmic beats Æ suspicion of a déhiscent vertical semicircular canal on both sides Æ confirmation by CT left left Pat. 1 Tullio Oszilopsie Hörminderung Autophonie Tinntius Hennebert Valsalva Schwindel Pat. 2 Pat. 3 Pat. 4 Pat. 5 Pat. 6 Pat. 7 Pat. 8 Pat. 1 Tullio Oszilopsie Hörminderung Autophonie Tinntius Hennebert Valsalva Schwindel Pat. 2 Pat. 3 Pat. 4 M.K.,1967 7th day after sugery Treatment proposition • Sealing of the dehiscence at first on the left side • In case of favorable outcome sealing also of the right sided dehiscence a few months later Æ the patient has not decided yet Vertigo and Tinnitus related to Stapes Hypermobility The two types of Tullio and Hennebert I Additional window in the vestib. labyrinth a) horizontal semi-circular canal Æ horizontal nystagmus (ev. rotat.) = classical fistula sign e.g. in cholesteatoma b) vertical semi-circular canal Æ vertical nystagmus II Stapes-Hypermobility (particularely in presence of a sacculo-utricular hydrops) Æ Jogger vertigo Æ Trumpet player vertigo Fistula Sign Vertigo and Nystagmus elicited by pressure on the ear mostly due to horizontal canal arrosion by an advanced cholesteatoma Hennebert Sign Fistula Sign without tympanic membrane perforation described initially in congenital syphilis, presently known as a classical sign of endolympatic hydrops Tullio Phänomen Vertigo and Nystagmus elicited by loud noise Case report 1: male, 46 years - Stapedotomy 4 years ago in an African country followed by profound deafness - Symptoms: - Vertigo, nausea and vomiting during jogging + pulsating tinnitus during jogging synchronous to the steps in the operated ear - Stapedectomy revision: - loose stapes prosthesis (figure 1) - absence of perilymph fistula - Treatment: - extraction of piston - closure of oval window with ear lobe fat - Follow up: - no more vertigo - no more tinnitus Case report 2: male, 40 years - Symptoms: Since two years vertigo, nausea and vomiting during jogging and wood-chopping + pulsating tinnitus in the left ear, synchronous with steps and physical aactivity - Hearing tests: - normal pure tone threshold - normal tympanometry and stapedial reflex measurements - Exploratory tympanotomy, left ear: - loose incudo-stapedial joint - striking stapes hypermobility - absence of perilymph fistula - Treatment: - Incus interposition - Follow up - Stop vertigo, stop tinnitus . Case report 3: woman, 50 years - Longstanding, conductive hearing loss (50 dB) in the left year following a longitudinal temporal bone fracture during childhood - Symptomes: After A substentional weight loss appearance of: vertigo, nausea and vomiting during forced respiration + pulsating tinnitus synchronous to respiratory movements in the left year - Ear examination striking Tympanic membrane movements synchronous to respiratory movements (evoking a flatulous Eustachian tube) - Hearing test: - Conductive hearing loss of 50 dB in the left ear - Exploratory tympanotomy left ear (Figure 3 a): - Complete fixation of malleus and incus - Striking hypermobility of stapes - Absence of perilymph fistula - Treatment: - Extraction of stapes - Extraction of incus - Extraction of malleus head - Stapedectomy with piston - Fixation on the malleus handle (figure 3b) - Follow up: - no More vertigo - no More tinnitus - Substantional postoperative hearing gain (remaining air bone-gap: 20 dB) Hennebert-Zeichen Fistelsymptom Schwindel und Nystagmus bei Druckausübung auf das Ohr meist Arrosion des lateralen Bogengangs durch ein Cholesteatom Tulliophänomen Schwindel und Nystagmus bei Lärmeinwirkung Fallvorstellung HNO R.C. 54-jährig, m. Anamnese: • Seit 1 Jahr intermittierender Drehschwindel, welcher jeweils während einigen Sekunden anhält, und durch Ausübung von Druck aufs linke Ohr ausgelöst wird. • Gelegentlich auch Schwindel bei kurz dauernder Druckveränderung (z.B. beim Zuschlagen einer Autotür im Innern des Autos) • Lärm führt nicht zu Schwindel Befund: • Valsalva-Manöver und Absaugen im äusseren Gehörgang links führen zu Drehschwindel mit horizontalem Nystagmus nach rechts • Weber mittelständig, Rinne bds. Pos. • RTA: Normakusis bds. • CT-Felsenbein unauffällig, insbesondere keine Dehiszenz des vertikalen Bogenganges. Schwindelphänomene o Hennebert-Zeichen Schwindel und Nystagmus durch pos. oder neg. Druck im äusseren Gehörgang o Tullio-Phänomen Schwindel und Nystagmus durch lauten Schall o Hypermobiler Stapes Schwindel und rhythmisches Ohrgeräusch bei rhythmischer körperlicher Aktivität Hennebert-Zeichen Schwindel und Nystagmus durch pos. oder neg. Druck im äusseren Gehörgang o Entspricht einem Fistelzeichen ohne Läsion im Mittelohr und ohne Fistel des Innenohrs o Auftreten bei kongenitaler Syphilis und beim M. Menière o Histologisch: Adhäsion des Utriculus und Sacculus zur Stapesfussplatte. o Ein hypermobiler Stapes verstärkt die Symptomatik Tullio-Phänomen Schwindel und Nystagmus durch lauten Schall o Typ I: zusätzliche Oeffnung gegen das Innenohr, z.B. durch eine Fistel zum lateralen Bogengang. o Typ II: hypermobiler Stapes, wobei beim Stapediusreflex eine Reizung des Utriculus oder Sacculus auftritt. Tullio-Phänomen Typ II Brandt 2000 Tullio-Phänomen Schwindel und Nystagmus durch lauten Schall o Spontanheilung beschrieben o Therapieoption bei hypermobilem Stapes: - Steigbügelkonsolidierung mit Fettgewebe, - Durchtrennung der Sehne des Stapediusmuskels - Stapedotomie Hypermobiler Stapes o Schwindel und rhythmisches Ohrgeräusch bei rhythmischer körperlicher Aktivität (Trompetenspieler, Jogger, Holzhacker) o Tullio-Phänomen Typ II o Verstärkung des Hennebert-Zeichens Fallvorstellung HNO R.C. 54-jährig, m. Diagnose: Schwindel mit positivem Hennebert-Zeichen Therapie: transkanaläre exploratorische Tympanotomie und Argon-LaserStapedotomie links Verlauf: 10d postop. Kontrolle war der Patient bei erhaltener Hörfähigkeit schwindelfrei. Case report I M.K., born 1967, MD • • • • Normal ENT examination Normal audiogram Normal vestibular testing Hennebert sign positive on the left (vertical nystagmic beats) • Normal classical CT of the head Æ suspicion of a dehiscent vertical semi-circular canal on the left right left right left right right