Spinale Tumore
Werbung

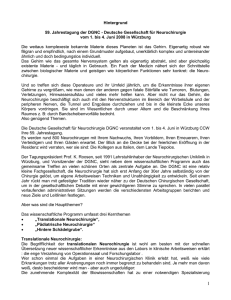
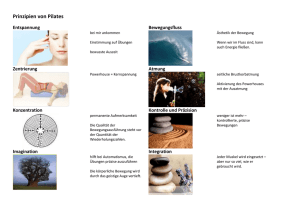
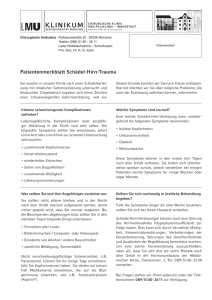
Operative Therapie bei Wirbelsäulenmetastasen !"#$%&'()$#$*$+,-( ./0*)&%1(* 0*) 2(1/$33&$,-4($5(* $* )(/ "*4"&"1$+,-(* 6(-%7$&$5%5$"* &'( )*+( ,-.'/*0- 1*23 45..*6 !"#$%&'()$#$*$+,-( 2(8(/50*1 $* )(/ 9*4"&"1$( %*-%*) :"* 2($+;$(&(* A. Alfieri, 2015 &'( )*+( 7/'8/9 7-'9*0:‐1*/6/:;<3 7=;>?@ !<';"+$0' = ‐ A?6B*'*6C'-=) D% E?+*'-9/?6# &'( F0'/>* 7-6+*)*'‐,'*=0/;<3 G?99.=: >"/4+-";? @0'"/)"40'(*5%5$"* A B&$*$+,-( B/(7+/(1$+5/$(/0*1 0*5(/ *(0(* 1(+(5#&$,-(* 2()$*10*1(* B/(7+3/C-(/4(**0*1+‐ 0*) /(1$+5(/1(+(5# DBE6.F ‐ >%+ G*)(/5 +$,- $' H%*) 2/%*)(*70/1I &'( '*'( )*+/;( I6*99 J/00-;>3 K'-6>B='9 LM+*'N J=K .=K L.6@K LM6@NNN ‐ >%+ $+5 8$,-5$1 7($ )(/ ="40'(*5%5$"* )(/ !5/%-&(*5-(/%;$(I &'( )*+( O9*P<-6 A?:@/83 7-+ O--'?@ !"#!! ‐ !$#!! !$#!! ‐ !$#7! !$#7! ‐ >>#7! %&'() 8,94 ?(&) Metastastische Wirbelsäulenerkrankungen • Häufigkeitzunahme (Verbesserung Diagnostik und Therapie der Grunderkrankung, demographische Entwicklung) • Unterschiedliche Präsentationen Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] EPIDURAL Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] INTRADURAL JUXTAMEDULLÄR Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] INTRADURAL JUXTAMEDULLÄR Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] INTRADURAL INTRAMEDULLÄR Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Operationstechniken bei spinalen Metastasen Mikrochirurgische Technik 7 Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Operationstechniken bei spinalen Metastasen Intraoperatives Neuromonitoring 9 Intraoperatives Monitoring (IOM) • • • • • falsch-positiv ca. 0,5 % / falsch-negativ ca. 1 % Spezifität / Sensitivität (MEPs, SSEPs): 95-99 % Monitoring bei deutlichen Defiziten eingeschränkt Monitoring während der gesamten OP unerlässlich Aber: IOM-induzierte Maßnahmen verhindern nur in ~ 50 % postoperative Defizite • Indiziert bei intramedullären Tumoren NeurochirurgieUpdate 2012 Klinik für Neurochirurgie und Wirbelsäulenchirurgie Spinale Tumore [email protected] Operationstechniken bei spinalen Metastasen Intraoperative 3D Bildgebung 11 • En bloc Spondylektomie Extraäsionale Resektion, kurativ,, extrem lang, Blutverluste (Eur Spine J 2010:19 231-241, Spine 1997: 22 324-327) • Vertebrektomie dorsale, thorakale Zugängen mit hohem Thrombose - und Infektionsrisiko (JNS Spine 2009 :111 272-279) • Wirbelkörperersätze distrahierbare Cages (Titan, PMMA) bessere Kyphosekorrektur (Eur Spine J 2011: 20 1369-1374) • Minimal-invasive Chirurgie, Tubuläre Zugänge geringer Blutverlust, kürzere VWD, geringe Morbidität, keine extraläsionale Resektion (JNS Spine 2011 :14 754-768) • Kyphoplastie, Elastoplastie ambulante Behandlung, sofortige Schmerzlinderung, Stabilität, diagnostisch, ideale Ergänzung RT (JNS Spine 2011 :14 754-768) Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] • Kyphoplastie, Elastoplastie ambulante Behandlung, sofortige Schmerzlinderung, Stabilität, diagnostisch, ideale Ergänzung RT (JNS Spine 2011 :14 754-768) Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] • En bloc Spondylektomie Extraäsionale Resektion, kurativ,, extrem lang, Blutverluste Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] radiographic artifact encountered on magnetic resonance imaging in the setting of proximate spinal instrumentation. The myelography and simulation are often performed prior to patient discharge from perioperaMassenreduktion (separation) tive hospitalization. Single-fraction (24 Gy) or hypofractionated SRS (typically 18–36 Gy in 3–6 fractions) A B C D E as extensions of the gross tumor volume to acco for the presumed microscopic disease extension adjacent marrow spaces (eg, the entire vertebral b when adjuvante only a proportion of the body is radiogra und Radiochirurgie 43 cally involved). The planning treatment volume 2- to 3-mm expansion of the clinical tumor volum F Fig 3. — Representative case of epidural spinal cord compression amenable to separation surgery plus radiosurgery. This 70-year-old man with meta renal cell carcinoma presented with severe neck pain and left upper extremity weakness. Panel A shows MRI (sagittal T1–gadolinium-enhanced). Pa (axial) demonstrates C6 metastasis with a burst fracture and extension into the posterior elements with circumferential epidural disease and highcord compression. Posterolateral instrumented fusion was performed with bilateral lateral mass screws at C3, C4, and C5, and with pedicle screws and T2. Laminectomy was performed at C5 to C7 and facetectomy at C6–7 bilaterally. The epidural tumor was circumferentially removed, including fro left-sided C6 and C7 nerve roots, as demonstrated on (C) postoperative myelogram and (D) MRI. Lateral radiographs demonstrate the hardware po (E). Adjuvant SRS (27 Gy in 3 fractions) was administered beginning on postoperative day 18. Hand strength was improved at the latest follow-up. P shows the dose distribution of image-guided radiation therapy. Planning target volume is depicted by the inner magenta line; the 95% isodose line is and the 50% isodose-exposed region is cyan. MRI = magnetic resonance imaging, SRS = stereotactic radiosurgery. 172 Cancer Control Klinik für Neurochirurgie und Wirbelsäulenchirurgie April 2014, Vol. 21, [email protected] Komplikationen? Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Komplikationen Kim et al., Spine. 2012; 37:78-84 • Systematische Literaturanalyse • 33 Studien 2.495 Patienten mit spinalen Met. • Komplikationsrate der OP: - gesamt: 29 % - infektiös: 8% - pulmonal: 4% - instrumentations-bezogen: 4 % Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Entscheidung zur Operation bei spinalen Metastasen - How I do it • Tokuhashi - Skala für OP Entscheidung • Tomita -Skala für chirurgisches Vorgehen Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] TOKUHASHI 68:213–218 nal instability neoplastic score: an analysis of relia0 Punkte 1 Punkt 2 Punkte 3 Punkte 5 (1990) Punkte 29. Tokuhashi Y, Matsuzaki 4 H, Punkte Toriyama S et al bility and validity from the spine oncology study Scoring system for the preoperative evaluation of group. J Clin Oncol 29:3072–3077 Karnofsky- 11. Gasbarrini 10–40 A, Li H, Cappuccio 50–70 80–100 M et al (2010) Effimetastatic spine tumor prognosis. Spine 15:1110– Index (%) cacy evaluation of a new treatment algorithm for 1113 spinal metastases. Spine 35:1466–1470 30. Tokuhashi Y, Matsuzaki H, Oda H et al (2005) A reExtraspinale 12. Ghogawala 3 oder mehr 1–2 0 Z, Mansfield FL, Borges LF (2001) Spivised scoring system for preoperative evaluation Knochennal radiation before surgical decompression adverof metastatic spine tumor prognosis. Spine 30: sely affects outcomes of surgery for symptomatic 2186–2191 metastasen metastatic spinal cord compression. Spine 26:818– 31. Tomita K, Kawahara N, Kobayashi T et al (2001) 3 oder mehr 2 1 Wirbelkörper- 824 Surgical strategy for spinal metastases. Spine 13. Harrington KD (1997) Orthopedic surgical mana26:298–306 metastasen gement of skeletal complications of malignancy. 32. Van der Linden YM, Dijkstra SPDS, Vonk EJA et al Frankel Frankel A/B Frankel C/D Frankel E(2005) Prediction of survival in patients with metaCancer 80:1614–1627 14. Huch K, Cakir B, Ulmar B et al (2005) Prognosis, stases in the spinal column: results based on a ranViszerale Nicht Resezierbar keine surgical therapy and progression in cervical and domized trial of radiotherapy. Cancer 103:320–328 upper-thoracic 33. Wai EK, Finkelstein JA, Tangente RP et al (2003) Metastasen resezierbartumor osteolysis. Z Orthop Ihre Quality of life in surgical treatment of metastatic Grenzgeb 143:213–218 Primärtumor15. Ibrahim Lunge, Magen, Leber, Andere Rektum, Prostata, spine Niere, disease. Spine 28:508–512 A, Crockard A, Antonietti P et al (2008) Do34. WangUterus JC, Boland P, Mitra N et al (2004) SingleesBlase, spinal surgery improve the quality of life for ÖsophaGallenblase, SchildKarzinoid stage posterolateral transpedicular approach for those with extradural (spinal) osseous metastases? gus, Pankreas, unbekannt drüse, resection of epidural metastatic spine tumors inAn international multicenter prospective obserOsteosarkom Mamma volving the vertebral body with circumferential revational study of 223 patients. Invited submission construction: results in 140 patients. Invited subfrom the Joint Section Meeting on Disorders of the mission from the Joint Section Meeting on DisorSpine and Peripheral Nerves, March 2007. J NeuroTab. 6 Interpretation des modifizierten Tokuhashi-Scores. [30]) ders(Nach of the Spine and Peripheral Nerves, March surg Spine 8:271–278 2004. J Neurosurg Spine 1:287–298 16. Jacobs WB, Perrin RG (2001) Evaluation and treatScore Überlebensprognose Empfehlung 35. Weigel B, Maghsudi M, Neumann C et al (1999) ment of spinal metastases: an overview. NeuromanagementTherapie of symptomatic spinal me11:e10 Gruppe A 0–8surg Focus 85% der Patienten überleben bis zu 6 Surgical Konservative oder palliatitastases. Postoperative outcome and quality of life. 17. Jensen MP, Chen C, Brugger AM (2002) PostsurgiMonaten ver chirurgischer Eingriff Spine 24:2240–2246 cal pain outcome assessment. Pain 99:101–109 36. Wibmer C, Leithner A, Hofmann G etEingriff al (2011) Sur18. Laufer I,73% Rubin der DG, Lis E et al (2013) The NOMS >6 MoGruppe B 9–11 Patienten überleben Palliativer chirurgischer oder vival analysis of 254 patients after manifestation of framework: approach to the treatment of spinal nate; 30% >12 Monate in Ausnahmefällen Tumorexzision metastatic tumors. Oncologist 18(6):744–751 spinal metastases: evaluation of seven preoperati19. Lee BH, 95% Kim T-H, Chong H-S et al (2013) Prognos->12 ve scoring systems. Spine 36:1977–1986 Gruppe C 12–15 der Patienten überleben Tumorexzision tic factor analysis in patients with metastatic spi37. Wiedenhöfer B, Möhlenbruch M, Hemmer S et al Monate Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] ne disease depending on surgery and conservati(2012) Vertebral stability in management of spinal Tab. 8 Interpretation des Tomita-Scores. (Nach [31]) Analysis Spinal metastases from solid tumors. of Blase, ÖsophaGallenblase, Uterus TOMITA SchildKarzinoid gus, Pankreas, unbekannt drüse, factors affecting survival. Cancer 76:1453–1459 Empfehlung veillance and Punkte ÜberlebenswahrTherapieziel Mamma Osteosarkom im 27. Taneichi H,scheinlichkeit Kaneda K, Takeda N et al (1997) Risk . Am J Med Mittel (Monate)of vertebral body collapse factors and probability des modifizierten Tokuhashi-Scores. (Nach [30]) Tab. 6 Interpretation 2–3metastases 50 of the thoracicLokale and lumbar spine. Ausgedehnte oder marginale (2010) A novelGruppe A in Score Überlebensprognose Langzeitkontrolle Empfehlung Exzision Spine 22:239–245 bility in neoGruppe BA 0–8 85%23,5 der Patienten überleben bis zu 6 lokale Konservative Therapieerreichende oder palliatiGruppe 4–5 Mittelfristige Tumorgrenzen 28. TeixeiraMonaten WGJ, Coutinho PR deKontrolle M, Marchesever LDchirurgischer etoder al intraläsionale pproach and Eingriff Exzision (2013) Interobserver agreement forMothe spine in- chirurgischer Eingriff oder cology Study Gruppe B 9–11 73%15der Patienten überleben >6 Palliativer Gruppe C 6–7 Kurzfristige lokale Palliativer Eingriff stabilitynate; neoplastic according intoAusnahmefällen the 30% >12 score Monatevaries Tumorexzision Kontrolle experience of the evaluator. Clinics Paulo) et al (2011) Spi-Gruppe Gruppe DC 12–15 Patienten überleben >12(Sao Tumorexzision 8–10 95%6 der Terminale VersorPalliative Maßnahmen, keine 68:213–218 nalysis of reliaMonate gungsphase operative Intervention 29. Tokuhashi Y, Matsuzaki H, Toriyama S et al (1990) Tab. 97 Überlebensprognose Faktoren zursystem Berechnung des Tomita-Scores. (Nach [31]) of (Nach [3]) Tab. nach dem modifizierten Bauer-Score. Scoring for the preoperative evaluation 1spine Punkttumor prognosis. 4 Punkte Punkte Einjahresüberleben (%)2 Punkte Empfehlung (2010) Effimetastatic Spine 15:1110– Primärtumor Langsames Wachstum Mäßiges Wachstum Rasches Wachstum (LunA 1113 4–5 50 Exzisionschirurgie algorithm for Gruppe Prostata, Uterus) Leber, Magen, Kolon, Gruppe B30. Tokuhashi 2–3 25Matsuzaki Palliativer Eingriff 470 Y,(Mamma, H, Oda H(Nieren, et al (2005) A re- ge, Schilddrüse) unklarer Primarius) 0–1 scoring 0 system for preoperative evaluation Keine operative Intervention LF (2001) Spi- Gruppe C vised Viszerale Metastasen Behandelbar Nicht behandelbar pression adverof metastatic spine tumor prognosis. Spine 30: Knöcherne Metastasen Solitär Multiple zur Berechnung des Van-der-Linden-Scores. (Nach [32]) symptomatic Tab. 10 Faktoren 2186–2191 Punkte 1 Punkt 2 Punkte 3 Punkte Spine 26:818– 31. Tomita0 K, Kawahara N, Kobayashi T et al (2001) 50–70 80–100 Surgical strategy for spinal metastases. Spine 728 | Karnofsky-Index Der Orthopäde 9 · 20–40 2013 (%) rgical mana26:298–306 Viszerale Ja Nein malignancy. 32. Van der Linden YM, Dijkstra SPDS, Vonk EJA et al Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Metastasen cology study Limitationen der Prognoseklassifikationen • Therapeutische Fortschritte • Individuelle (genetische) Unterschiede Tumorboards (Einzelfallentscheidung) NeurochirurgieUpdate 2012 Klinik für Neurochirurgie und Wirbelsäulenchirurgie Spinale Tumore 22 [email protected] Metastastische Wirbelsäulenerkrankungen • OP Entscheidung (OP-Nutzen vs. OP-Risiko) • Art der Operation (minimal vs maximal) • Prognose als entscheidender Faktor • Einzelfallentscheidung / Tumorboards Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected] Danke für Ihre Aufmerksamkeit! Klinik für Neurochirurgie und Wirbelsäulenchirurgie Hochschulklinikum der Medizinischen Hochschule Brandenburg Ruppiner Kliniken Klinik für Neurochirurgie und Wirbelsäulenchirurgie [email protected]