Chronische Erschöpfung - Ätiologie, Diagnostik und Therapie.
Werbung

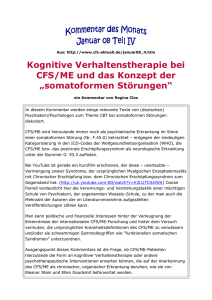
Chronische Erschöpfung - Ätiologie, Diagnostik und Therapie. Vortrag am Universitätsspital Basel PD Dr. phil. Jens Gaab Klinische Psychologie und Psychotherapie, Psychologisches Institut, Universität Zürich [email protected] Prävalenz von Erschöpfung Prävalenz von Erschöpfung Fachärzte / Kliniken Medizinische Erstversorgung Allgemeinbevölkerung 0 10 Chronisches Erschöpfungssyndrom 20 30 40 50 Chronische Erschöpfung (über 6 Monate) 60 70 80 Andauernde Erschöpfung (über 1 Monat) Ursachen von Erschöpfung E Beispiel: Interferonbehandlung bei Karzinomerkrankung Beispiel: Rheumatoide Arthritis Direkte Folge der Erkrankung Nebenwirkung der Medikation Akute / chronische Belastungen r s c h Psychische Störungen (vor allem Depressive Störungen und Angststörungen ö p f u n Mit komorbiden psychischen Störung (vor allem: Depressive Störungen und Angststörungen) Symptom Somatisch ohne komorbide psychische Störung Eigenständige Störung Psychisch Ursache g bei adäquater medikamentöser Behandlung einer bestehenden somatischen Erkrankung Definitionskriterien Chronic Fatigue Syndrome (CFS) Was sind somatoforme Störungen? Definition somatoformer Störungen "Das Charakteristikum ist die wiederholte Darbietung körperlicher Symptome in Verbindung mit hartnäckigen Forderungen nach medizinischen Untersuchungen trotz wiederholter negativer Ergebnisse und Versicherung der Ärzte, dass die Symptome nicht körperlich begründbar sind. Wenn somatische Störungen vorhanden sind, erklären sie nicht die Art und das Ausmaß der Symptome, das Leiden und die innerliche Beteiligung des Patienten." ICD-10, Internationale Klassifikation der Krankheiten, 10. Revision (WHO) "Das gemeinsame Merkmal der Somatoformen Störungen ist das Vorhandensein von körperlichen Symptomen, die einen medizinischen Krankheitsfaktor nahelegen und die durch einen medizinischen Krankheitsfaktor nicht vollständig erklärt werden können." DSM-IV-TR, Diagnostisches und Statistisches "körperliche symptome, die nicht körperlich begründbar sind" grundannahme: somatoforme symptome letztendlich die somatische manifestationen psychischer störungen sind. Exkurs Sind somatoforme Störungen bedeutsam? Patienten mit somatoformen Störungen haben im Vergleich zu Patienten ohne somatoforme Störungen eine doppelt so hohe Inanspruchnahme medizinischer Leistungen und verursachen doppelt so hohe Kosten. Barsky et al., 2005, Archives of General Psychiatry 30-50% der Patienten mit somatoformen Störungen haben krankheitsbedingte Arbeitsausfälle. Lieb et al., 2000, Acta Psychiatrica Scandinavica die zweite frage ist, ob ss eigentlich bedeutsam ist. hier exemplarisch zwei sehr gute studien, die da eine einschätzung ermöglichen. beispielsweise konnte barsky und mitarbeiter an patienten in der allgemeinarzt-praxis. sie fanden, dass patienten mit somatoformen störungen eine doppelt so hohe inanspruchname medizinischer leistungen aufwiesen und als folge auch doppelt so hohe kosten verursachten. entsprechend konnten lieb und mitarbeiter zeigen, dass zwischen 30-50% aller jugendlichen und jungen erwachsenen mit somatoformen störungen krankheitsbedingte arbeitsoder schulausfälle aufwiesen. wichtig ist, dass diese beiden befunde nicht durch das vorliegen von anderen psychischen störungen, wie angststörungen oder depressionen, bedingt waren. Klassifikation somatoforme Störungen Aktuell, Probleme und Änderungsvorschlag Somatisierungsstörung Undifferenzierte somatoforme Störung Konversionsstörung Körperdysmorphe Störung Hypochondrie Schmerzstörung Somatoforme Störung NNB Mayou et al., 2005, American Journal of Psychiatry Klassifikation somatoforme Störungen Aktuell, Probleme und Änderungsvorschlag Angststörungen Somatisierungsstörung Undifferenzierte somatoforme Störung Körperdysmorphe Störung Gesundheitsangst Konversionsstörung Schmerzstörung Somatoforme Störung NNB Mayou et al., 2005, American Journal of Psychiatry Klassifikation somatoforme Störungen Aktuell, Probleme und Änderungsvorschlag Angststörungen Somatisierungsstörung Undifferenzierte somatoforme Störung Körperdysmorphe Störung Gesundheitsangst Dissoziative Störungen Konversionsstörung Schmerzstörung Somatoforme Störung NNB Mayou et al., 2005, American Journal of Psychiatry Klassifikation somatoforme Störungen Aktuell, Probleme und Änderungsvorschlag Angststörungen Persönlichkeitsstörungen Undifferenzierte somatoforme Störung Körperdysmorphe Störung Somatisierungsstörung Gesundheitsangst Dissoziative Störungen Konversionsstörung Schmerzstörung Somatoforme Störung NNB Mayou et al., 2005, American Journal of Psychiatry Klassifikation somatoforme Störungen Aktuell, Probleme und Änderungsvorschlag Angststörungen Körperdysmorphe Störung Persönlichkeitsstörungen Somatisierungsstörung Gesundheitsangst Dissoziative Störungen Konversionsstörung Medizinische Funktionell somatische Symptome Mayou et al., 2005, American Journal of Psychiatry Klassifikation Funktionelle Somatische Syndrome ilat lv ic me dro lS yn e we Bo ble Pe ita c pep ent ni Dys c i n o Fa ue g ti S d n y r om ac ead he hr i C nH n Syn o i s Merkmale. droFunctionalTen me Fibromyalgia Somatic Chronic Low Back Pain me o Mu r d Syndromes ltip n n y i S le C a l P a P r u h em r e t l m ns a ica e i m en c l Se e r a P nsit F s t l ivit r uDa y ca i yl s p ph ty A or iDc is or de r er cia te dD so As as h ipl rd aisro buDl ndi a om Wh por Tem rde r Unexplained Chest Pain Pa iso ion sia Problem IV. Gleiche Therapien wirken. erv ro nal Problem III. Gleiche nicht-symptomatische Hyp ctio Problem II. Patienten überlappen. Ch Irr Fun Problem I. Definitionen überlappen. Globus Hystericus Funktionelle somatische Syndrome - One or many? Wessely et al., 1999, The Lancet Psyche Psychobiologisches Erklärungsmodell langfristig Sozialisations- / Entwicklungsbedingungen Eigene Ziele werden nicht mehr erreicht Somatisches subjektives Krankheitsmodell kurzfristig Niedriger Selbstwert Orientierung an externer Bewertung Vermeiden von Schwäche Angst vor Zurückweisung Perfektionismus Leistungsorientierung Überlastung Kompensatorische Anstrengung bursts of activity Depressionen Ängste Depressionen Ängste Stressbedingte somatische Veränderungen Anlage stör ungsun- = individuumsspezifische Pr ozesse Inaktivität Schlafstörungen Chronische Symptome Sekundäre somatische Veränderungen Infektion Symptome Fokus auf Symptome Somatische Beschwerden Geringe Belastbarkeit Entwicklung somatischer Symptome Soma Anpassung Verzögerte Rekonvaleszenz Auslösung Aufr echter haltung stör ungsspezifische Pr ozesse Psychobiologisches Erklärungsmodell Hormonelle Reaktivität auf pharmakologischen Stress (ITT) bei Patienten mit chronischem Erschöpfungssyndrom ACTH nach pharmakologischem Stress Gaab et al., 2002, Psychosomatic Medicine 1400 1200 1000 800 600 400 200 0 Patienten Gesunde Psychobiologisches Erklärungsmodell Zusammenhänge zwischen hormonellen Veränderungen und psychischen Belastungen bei Patienten mit chronischem Erschöpfungssyndrom r=-0.63, p=0.003 gering Ausmass der hormonellen Dysregulation (ACTH) hoch gering hoch Ausmass der psychischen Belastung Psyche Psychobiologisches Erklärungsmodell langfristig Sozialisations- / Entwicklungsbedingungen Eigene Ziele werden nicht mehr erreicht Somatisches subjektives Krankheitsmodell kurzfristig Niedriger Selbstwert Orientierung an externer Bewertung Vermeiden von Schwäche Angst vor Zurückweisung Perfektionismus Leistungsorientierung Überlastung Kompensatorische Anstrengung bursts of activity Depressionen Ängste Depressionen Ängste Stressbedingte somatische Veränderungen Anlage stör ungsun- = individuumsspezifische Pr ozesse Inaktivität Schlafstörungen Chronische Symptome Sekundäre somatische Veränderungen Infektion Symptome Fokus auf Symptome Somatische Beschwerden Geringe Belastbarkeit Entwicklung somatischer Symptome Soma Anpassung Verzögerte Rekonvaleszenz Auslösung Aufr echter haltung stör ungsspezifische Pr ozesse Erklärungsmodell - Fokus auf Persönlichkeit Table 2. Logistic Regression Models Estimating the Likelihood of Having CFS Relative to Childhood Trauma Exposure in CFS Cases and NF Controls Identified From the General Population in Wichita, Kan* 100 NF (n = 60) OR (95% CI) CDC SI Scores Any category Yes No Emotional abuse Yes No Physical abuse Yes No Sexual abuse Yes No Emotional neglect Yes No Physical neglect Yes No CFS (n = 43) P Value† 27 (63) 16 (37) 22 (37) 38 (63) 3.35 (1.43-7.88) 1.00 .006 18 (42) 25 (58) 12 (20) 48 (80) 2.87 (1.19-6.70) 1.00 .02 12 (28) 31 (72) 6 (10) 54 (90) 4.28 (1.35-13.60) 1.00 .01 12 (28) 31 (72) 3 (5) 57 (95) 8.00 (2.02-31.70) 1.00 .003 26 (60) 17 (40) 17 (28) 43 (72) 4.58 (1.90-11.00) 1.00 .001 7 (16) 36 (84) 2 (3) 58 (97) 5.90 (1.15-30.30) 1.00 .03 Abbreviations: CFS, chronic fatigue syndrome; CI, confidence interval; † 60 ∗ 40 ∗ 20 0 † Total Case Definition Frequency Intensity Symptom Number Figure. Childhood trauma and the severity of chronic fatigue syndrome (CFS). Mean Centers for Disease Control and Prevention Symptom Inventory (CDC SI) scores are shown as a function of exposure to childhood trauma in cases with CFS. Error bars reflect standard error of the mean. *P!.01. †P!.05. an elevated risk for CFS even in the presence of low levels of psychopathology. Risk for CFS increased further in the presence of high levels of psychopathology. Table 1. Mean CTQ Scores in CFS Cases and NF NF, Controls Identified nonfatigued; OR, odds From ratio. the General Population in Wichita, Kan CTQ Score ∗ 80 No. (%) Above the Cutoff Predictor CFS With Early Trauma (n = 27) CFS Without Early Trauma (n = 16) COMMENT *Exposure to childhood trauma was based on the following Childhood Trauma Questionnaire cutoff scores for moderate-to-severe trauma40: We explored associations between CFS and multiple Mean Score (95% emotional abuse, "13;CI) physical abuse, "10; sexual abuse, "8; emotional P forms of childhood trauma and psychopathology using neglect, "15; and physical neglect, "10. All models were adjusted for age, CFS (n = 43) sex, and race. NF (n = 60) Statistic, F1,102dimensional rating Value scales in clinically confirmed CFS †Based on Wald #2 tests. cases compared with.001 controls identified from the population. Childhood trauma was an important risk factor .01 for CFS and the association demonstrated a graded .002 response. Childhood trauma was associated with CFS !.001 severity and symptoms .006 of depression, anxiety, and PTSD. Risk of CFS as a function of childhood trauma !.001 sion (z=6.46; P!.001). Significantly more CFS cases had increased with altered emotional state. Our findings are high state anxiety ("75th percentile) and met the cutin agreement with previous studies in tertiary care Abbreviations: CFS, chronic fatigue syndrome; CI, confidence interval; CTQ, Childhood Trauma Questionnaire; NF, nonfatigued. Heim etanal., 2006 Arch Gen Psychiat. off score for clinically significant PTSD compared with patients that found association between CFS and vic27 controls. Clinically relevant symptoms of depression and timization starting in childhood or exposure to PTSD were noted only in CFS cases and not in controls. adverse parenting.28 We also confirm and extend findTo examine the effect of psychopathology in moderating the ASSESSMENT OF PSYCHOPATHOLOGY In the Diagnostic Interview Schedule for DSM-IV, a ings suggesting that childhood abuse predicts PTSD CFSthan related to childhood exposure, we strati- with chronic fatigue.31 Our greater proportion of risk CFS of cases controls were di- trauma symptoms in individuals fied the CFS group basis of low vs high levels of psyLifetime and current DSM-IV Axis I psychiatric disorders agnosed as having current (7 cases [16%] on vs 1the control results are concordant with the findings from commuchopathology. We then used multinominal logistic regression P = .009) nity surveys reporting elevated rates of fatigue in were assessed using the Diagnostic Interview [2%]; Schedule for and lifetime (13 cases [30%] vs 5 con35 trols [8%]; P = .004) anxiety disorders, including PTSD, women experience25,26 and with analysis to estimate risk of belonging to eitherwith casechildhood group as abuse a DSM-IV. We diagnosed psychiatric disorders that are not whereasmajor there was only a trend increased lifetime studies that identified trauma as a risk factor function offor childhood trauma. The level of significance waschildhood set exclusionary for CFS,3,34 including nonmelancholic major depression. for functional somatic syndromes in general.44-49 We at P!.05 for all tests. depression, anxiety disorders, and PTSD. We measured curwere significant correlations between the overalso confirmed the well-known relationship between rent symptom severity using psychometricallyThere validated Emotional abuse Physical abuse Sexual abuse Emotional neglect Physical neglect Total score 10.6 (8.9-12.4) 7.7 (6.8-8.5) 10.8 8.0 (6.8-9.2) 6.5 (6.0-6.9) 6.85 8.0 (6.5-9.6) 5.7 (5.1-6.3) 9.89 Subjects with CFS reported more psychopathology 12.1 (10.3-13.9) 8.1 (7.2-9.0) 19.1 Table 3 ). Relative to controls, a than did NF controls ( 7.1 (6.3-8.0) 5.9 (5.5-6.3) 7.82 greater proportion of CFS cases had more severe depres45.9 (39.9-51.9) 33.9 (31.5-36.3) 17.3 Erklärungsmodell - Ursache der Ursachen CFS als (formale, nicht inhaltliche) Persönlichkeitsstörung. .......die Haltungen, Gefühle und Verhaltensweisen, welche die somatoforme Störung kennzeichnen, sind Folgen einer Störung bzw. Dysfunktion von wichtigen Bereichen der Persönlichkeit (Bass & Murphy, 1995). Anlage Beginn der Beschwerden Probleme Aufrechterhaltung Probleme Lösungsversuche + Lösung der Probleme - Vulnerabilität Lösungsversuche + Lösung der Probleme - Aufrechterhaltung Erklärungsmodell - Implikationen für Therapie Störungsunspezifische bewältigungs- und klärungsorientierte Interventionen Funktionaler Zusammenhang Störungsspezifische Prozesse Ressourcenaktivierung Störungsunspezifische Prozesse Störungsspezifische bewältigungs- und klärungsorientierte Interventionen Gaab & Ehlert, 2005 Behandlungsmodelle funktioneller somatischer Störungen http://www.openlibrary.org/details/ psychictreatment00duboiala welche implikationen hat eine biopsychosoziale perspektive auf die behandlung? auch hier wieder ein ausflug in die vergangenheit. ich bin dabei auf die arbeit von paul dubois gestossen, einen neuropathologie professor aus bern aus dem jahr 1904. er schreibt, und dass finde ich erstaunlich, "xxxxx". basierend auf diesem integrativen verständnis postuliert dubois vier prinzipien seiner psychischen therapie, welche wie folgt lauten XXXX. ist dieser fokus auf einem vertrauensvollem, akzeptierenden, erwartungsinduziertenden und kollaborativen verhältnis zwischen arzt und patient tatsächlich nachweisbar? ich möchte hier anmerken, dass herr Professor dubois sich hier tatsächlich selbst in einem gewissen dilemma sah, wie die folgenden zeilen aus dem vorwort seines buch belegen: XXXX Behandlungsmodelle funktioneller somatischer Störungen Dubois, 1908, The psychic treatment of nervous disorders, S. 41 welche implikationen hat eine biopsychosoziale perspektive auf die behandlung? auch hier wieder ein ausflug in die vergangenheit. ich bin dabei auf die arbeit von paul dubois gestossen, einen neuropathologie professor aus bern aus dem jahr 1904. er schreibt, und dass finde ich erstaunlich, "xxxxx". basierend auf diesem integrativen verständnis postuliert dubois vier prinzipien seiner psychischen therapie, welche wie folgt lauten XXXX. ist dieser fokus auf einem vertrauensvollem, akzeptierenden, erwartungsinduziertenden und kollaborativen verhältnis zwischen arzt und patient tatsächlich nachweisbar? ich möchte hier anmerken, dass herr Professor dubois sich hier tatsächlich selbst in einem gewissen dilemma sah, wie die folgenden zeilen aus dem vorwort seines buch belegen: XXXX Behandlungsmodelle funktioneller somatischer Störungen Prinzipien der psychischen Therapie, Dubois 1908 I. Aufbau einer vertrauensvollen Beziehung zwischen Behandler und Patient und Anerkennung der Sichtweise des Patienten II. Krankheitsgeschichte des Patienten (ohne Ungeduld) erfassen III.Professionelle Autorität und therapeutische Beziehung dazu nutzen, den Patienten von den Möglichkeiten einer Besserung überzeugen IV.Kollaborative Beziehung zwischen Behandler und Patient welche implikationen hat eine biopsychosoziale perspektive auf die behandlung? auch hier wieder ein ausflug in die vergangenheit. ich bin dabei auf die arbeit von paul dubois gestossen, einen neuropathologie professor aus bern aus dem jahr 1904. er schreibt, und dass finde ich erstaunlich, "xxxxx". basierend auf diesem integrativen verständnis postuliert dubois vier prinzipien seiner psychischen therapie, welche wie folgt lauten XXXX. ist dieser fokus auf einem vertrauensvollem, akzeptierenden, erwartungsinduziertenden und kollaborativen verhältnis zwischen arzt und patient tatsächlich nachweisbar? ich möchte hier anmerken, dass herr Professor dubois sich hier tatsächlich selbst in einem gewissen dilemma sah, wie die folgenden zeilen aus dem vorwort seines buch belegen: XXXX was not easy, and the resources of many of were exhausted in connection with him." In conclusion my confrere asked my my acquaintances advice upon some he might obtain the same results in his medical practise, which he was just beginning. I answered him by a long letter, in which I tried to bring out the peculiarities of the psychic treatment which I had used; but I had to point out to my friend that it was impossible for me to condense in such a way the experiences that had been gathered during more than twenty years, chiefly points, in order that Behandlungsmodelle funktioneller somatischer Störungen was only by personal conversations that he was able to see my views and put them into such form that he could use them in his practise. On the other hand, some intelligent patients among my colleagues, with whom I have had very friendly relations, have often expressed a desire to read what I had said to them. devoted to the treatment of the neuroses. I It have held out for a long time against these friendly We a period of exact research, of laboratory work, and of statistics that are more or less convincing, and I can offer only impressions and opinions which are based entreaties. upon what live in be conscientious observations, and on reflections which are forced upon me by facts, but I do I believe to not possess the necessary scientific reputation to insure their acceptance. in spite of these justifiable fears, I dare to face the criticism of my colleagues, it is first because I feel that I am If, Dubois, 1908, The psychic treatment of nervous disorders, Vorwort welche implikationen hat eine biopsychosoziale perspektive auf die behandlung? auch hier wieder ein ausflug in die vergangenheit. ich bin dabei auf die arbeit von paul dubois gestossen, einen neuropathologie professor aus bern aus dem jahr 1904. er schreibt, und dass finde ich erstaunlich, "xxxxx". basierend auf diesem integrativen verständnis postuliert dubois vier prinzipien seiner psychischen therapie, welche wie folgt lauten XXXX. ist dieser fokus auf einem vertrauensvollem, akzeptierenden, erwartungsinduziertenden und kollaborativen verhältnis zwischen arzt und patient tatsächlich nachweisbar? ich möchte hier anmerken, dass herr Professor dubois sich hier tatsächlich selbst in einem gewissen dilemma sah, wie die folgenden zeilen aus dem vorwort seines buch belegen: XXXX Behandlungsmodelle funktioneller somatischer Störungen Wirkfaktoren zur Erklärung von Psychotherapie-Effekten Erwartung 15% Extratherapeutische Veränderung 40% Therapiebeziehung 30% Störungsspezifische Techniken 15% Lambert & Barley, 2002, Research summmary on the therapeutic relationship and psychotherapy outcome, Kap. 2 in: Norcross, Psychotherapeutical relationships that work. Thomas -studie es muss hier angemerkt werden, dass ein immer noch inoffizielles definitionskriterieum der somatoformen störung ein schlechtes artt-patienten verhhältnis ist.. und man kann sich nun vorstellen, ob dies für eine behandlung eine gute voraussetzung darstellt. CHAPTER XVIII Behandlungsmodelle funktioneller The somatischer Störungen Rational Psychotherapy Its Efficacy in All Domains of Medicine The Necessity for Impressing the Patient with the Conviction of Cure Blind Faith and Rational Faith to Establish the Idea of Persistence_that Cure is Organic Complications Necessary Contrary Necessity of Changing the Mental State of the Sub- Suggestions ject Favorable Conditions for Attaining THE psychotherapy which this End has no need of I call rational this sort of preparatory narcosis of hypnosis, or of this Wirkfaktoren zur Erklärung von Psychotherapie-Effekten suggested. suggestibility that is It is itself hypernot addressed to an impressionable polygon, but simply to the mind and the reason of the subject. This psychic therapy is indicated in all the affections in which one recognizes the influence of Erwartung mental representations or ideas, and they are legion. 15% a great mistake to believe that psychic therapy is applicable only to psychoneuroses, that it is an aid for the It is neurology and the alienist alone, and that the Moral influence nearly always practitioner can pass it by. comes in, and ever since medicine has existed patients and Extratherapeutische Veränderung physicians have been able to prove it. It is not unusual 40% to specialist in see the patient's condition improve immediately after the visit of the physician, either as a consequence of the favorable Therapiebeziehung assurances that he has expressed, 30% he shows to his through all patient. or from the sympathy which This psychotherapy has existed To know how time. to apply it has always been Dubois, 1908, psychic treatment of nervous whoThe <are also the highest quality of those practitioners sicians of the soul, and who have known phy- how to acquire and) and appreciative clientele. Techniken keep a confiding Störungsspezifische They are, perhaps, more numerous in the country 15% and small towns than in great centers, tends to make Surgery influence. where competition develops mercantilism and the physician forget his humanitarian calling. on the therapeutic and psychotherapy outcome, Kap. 2 in: Norcross, Without relationship and the operation doubt, the diagnosis Psychotherapeutical relationships that work. itself Lambert & practised Barley, 2002, Research could not be without this moralsummmary Thomas -studie es muss hier angemerkt werden, dass ein immer noch inoffizielles definitionskriterieum der somatoformen störung ein schlechtes artt-patienten verhhältnis ist.. und man kann sich nun vorstellen, ob dies für eine behandlung eine gute voraussetzung darstellt. Probleme bei der Umsetzung Funktionelle somatische Symptome aus Sicht von Arzt und Patienten Je weniger lokalisierbar und spezifisch die Symptomatik, desto problematischer werden Patienten vom Arzt wahrgenommen Raine et al., 2004, British Medical Journal Erklärungen des Arztes werden vom Patienten meist als Ablehnung oder Widerspruch eigener Annahmen wahrgenommen Salmon et al., 1999, British Medical Journal Die meisten Patienten mit funktionellen somatischen Symptomen bekommen medizinische Behandlungen, ohne diese verlangt zu haben Ring et al., 2004, British Medical Journal Refused n = 33 (17%) Stage 1 assessment n = 160 randomisation Therapie - Evidenzen Counselling n = 80 months (SD = 41) and their mean fatigue score was 23.2 (SD = 5). All patients assessed met operational criteria fatigue13. Forty-five (28%) met operational criteria for the chronic fatigue syndrome. Six patients belonged to the Myalgic Encephalitis (ME) Association, all of whom met the criteria for CFS. Follow-up CBT n = 80 At three months the mean fatigue scores had fallen to 15.6 25 Received six sessions of therapy n = 55 Dropped-out of therapy n = 25 (31%) Lost to follow-up n = 15 Lost to follow-up n = 16 Completed all measures n = 65 (81%) Completed all measures n = 64 (80%) Figure 1. Trial profile. o Fatigue score Received six sessions of therapy n = 51 Dropped-out of therapy n = 29 (36%) ! 20 15 ! o o 3 Months 6 ! 10 0 Figure 2. Mean fatigue scores (with 95% CI) at baseline, three months and six months for patients randomised to CBT and counselling. - counselling; o - CBT. ! TableKVT 1. Patients whoDeale completed vs. PMR. et al., measures 1997 Am Jat 6 months compared with those who did not complete measures. Psychiat. Variable aLower KVT vs. Beratung/GT. Ridsdale et al.,Difference 2001 Brit(95% J Gen Completers Non-completers CI)Pract. (n = 129) (n = 31) scores denote improvement on all measures except the physical Male patients 34 (26%) 9 (29%) -2.7 (-20.4–15.0) functioning scale of the Medical Outcomes Study Short-Form General Mean age (years) 40.0 (SD = 13.6) 37.2 (SD = 13.5) 2.8 (-2.6–8.2) Fatigue atHealth baseline (mean) 23.2 (SD = 5.0) 23.8 (SD = 5.0) -0.64 (-2.7–1.4) Survey. Durationbof fatigue (mean number of months) 39.8 (SD = 43.0) 31.2 (SD = 29.0) 6.5 (-4.4–21.6) Three patients receiving cognitive behavior therapy and four patients History of anxiety and depression (from doctors’ notes) 7.3 (-12.2–26.8) Outcome-Prädiktor. Emotionale Prozessierung: Varianzaufklärung (Godfrey et al., Yes (59%) 16 (52%) receiving relaxation dropped out26% of76the study. No Anxiety score (mean) Depression score (mean) On antidepressant treatment at baseline Social adjustment score (mean) Patient’s beliefs of cause Physical or mainly so Psychological or mixed Met CFS criteria 53 (41%) 9.9 (SD = 4.4) 7.6 (SD = 3.8) 27 (21%) 19.3 (SD = 7.0) 15 (48%) 8.8 (SD = 4.4) 7.5 (SD = 3.8) 6 (19%) 20.5 (SD = 7.4) 62 (48%) 67 (52%) 37 (29%) 20 (67%) 10 (33%) 8 (26%) 1.1 (-0.7–2.9) 0.8 (-1.4–1.6) 1.6 (-0.1–0.2) -1.2 (-4.2–1.9) -18.6 (-37.5–0.34) 2.9 (-14.4–20.1) yards, bending, lifting, and climbing stairs). At 6-month xation exercises overly British Journal of General Practice, January 2001 21 follow-up, this had increased to 85.1 (able to carry out ing cognitive behavior Literatur Gaab & Ehlert (2005). Chronische Erschöpfung und Chronisches Erschöpfungssyndrom, Fortschritte der Psychotherapie, Hogrefe Verlag. Gaab (2005). Psychotherapie chronischer Erschöpfungszustände. Psychotherapeut Prins et al (2006). Chronic Fatigue Syndrome. Lancet Review 8FJUFSVOE'PSUCJMEVOH 1TZDIPUIFSBQFVUro %0*T 0OMJOFQVCMJ[JFSU0LUPCFS ª4QSJOHFS.FEJ[JO7FSMBH 3FEBLUJPO 6&IMFSUr;àSJDI 1-+BOTTFOr%PSUNVOE +(BBC ,MJOJTDIF1TZDIPMPHJFVOE1TZDIPUIFSBQJF1TZDIPMPHJTDIFT*OTUJUVUEFS6OJWFSTJUÊU;àSJDI Chronic fatigue syndrome 1TZDIPUIFSBQJFDISPOJTDIFS &STDIÚQGVOHT[VTUÊOEF Judith B Prins, Jos W M van der Meer, Gijs Bleijenberg Lancet 2006; 367: 346–55 Departments of Medical Psychology (J B Prins PhD) and Internal Medicine (J W M van der Meer MD) and Expert Centre for Chronic Fatigue (G Bleijenberg PhD), Radboud University Nijmegen Medical Centre, Nijmegen, Netherlands Correspondence to: Dr Judith B Prins, Radboud University Nijmegen Medical Centre, 840 Department of Medical Psychology, PO Box 9101, 6500 HB Nijmegen, Netherlands [email protected] ;VTBNNFOGBTTVOH $ISPOJTDIF&STDIÕQGVOHJTUFJOFEFSIÅVGJHTUFO#FTDIXFSEFOJOEFS"MMHFNFJOCFWÕMLF SVOH&STDIÕQGVOHJTUQFSTFFJOVOTQF[JGJTDIFT4ZNQUPNVOELBOO'PMHFWFSTDIJFEFOFS NFEJ[JOJTDIFS&SLSBOLVOHFOVOEQTZDIJTDIFS4UÕSVOHFOTFJO,ÕOOFOEJFTFBMT6STBDIF BVTHFTDIMPTTFOC[X[VS&SLMÅSVOHEFS#FTDIXFSEFOOJDIUWPMMTUÅOEJHIFSBOHF[PHFOXFS EFOLBOOEJF%JBHOPTFs$ISPOJTDIFT&STDIÕQGVOHTTZOESPNAtDISPOJDGBUJHVFTZOESP NFi$'4 WFSHFCFOXFSEFO8BTJTU$'4 8FMDIFO8FSUIBUEJFTF4UÕSVOHTLBUFHPSJF "VT HFIFOEWPOFJOFNQTZDIPCJPMPHJTDIFO7FSTUÅOEOJTTPMMFOQTZDIPUIFSBQFVUJTDIF"OTBU[ QVOLUF[VS#FIBOEMVOHDISPOJTDIFSTDIÕQGUFS1BUJFOUFOCFTDISJFCFOXFSEFO 4DIMàTTFMXÚSUFS $ISPOJTDIF&STDIÕQGVOHp$ISPOJTDIFT&STDIÕQGVOHTTZOESPNp1TZDIPUIFSBQJFp ¨UJPMPHJFNPEFMMp6OTQF[JGJTDIFT4ZNQUPN 1TZDIPUIFSBQZPGDISPOJDGBUJHVFTUBUFT "CTUSBDU $ISPOJDGBUJHVFJTDPNNPO4JODFGBUJHVFIBTMJUUMFTQFDJGJDJUZJUDBOCFUIFDPOTFRVFODF PGNBOZEJGGFSFOUTPNBUJDEJTFBTFTBOEQTZDIJBUSJDEJTPSEFST5IFSBQZOFFETUPCFJOEJ WJEVBMMZUBJMPSFEXJUISFHBSEUPUIFVOEFSMZJOHPSBTTVNFEDBVTFT8IFOPCKFDUJWFBOE FTUBCMJTIFEDBVTFTDBOOPUCFJEFOUJGJFEPSDBOOPUBEFRVBUFMZFYQMBJOUIFTZNQUPNTFYQF SJFODFEUIFEJBHOPTJTPGDISPOJDGBUJHVFTZOESPNF$'4 JTQPTTJCMF#VUXIBUJT$'4 *TJUBWBMJEEJBHOPTJT )PXDBOUIFDISPOJDGBUJHVFQBUJFOUCFUSFBUFE #BTFEPOBOJOUF HSBUJWFVOEFSTUBOEJOHBQTZDIPCJPMPHJDBMFUJPMPHJDBMBOEQTZDIPUIFSBQFVUJDBMNPEFMPG DISPOJDGBUJHVFXJMMCFEFWFMPQFEBOEEFTDSJCFE Chronic fatigue syndrome (CFS) is the term that is generally accepted by scientists and mostly by clinicians for the range of complaints that patients commonly refer to as myalgic encephalomyelitis (ME) or chronic fatigue and immune dysfunction syndrome. CFS is characterised by persistent and unexplained fatigue resulting in severe impairment in daily functioning. Sporadic CFS-like cases and epidemics were described first in the 19th and 20th centuries,1 but interest in CFS increased in the early 1980s with the advent of ME, a term that had been introduced 30 years earlier for an epidemic of neurological symptoms among staff at the Royal Free Hospital in London, UK. In the illness ME, apart from neurological symptoms, chronic fatigue was a main symptom. Initially, comparisons with neurasthenia were made,2 and a possible role of viruses and other microorganisms was examined.3–6 In the absence of a recognisable cause, ME was referred to as a psychiatric disorder7 or a 20thcentury illness. Controversial views about the dichotomy of organic versus functional were presented.8 Since then, practitioners have disagreed on Search strategy and selection criteria We searched the Cochrane Database of Systematic Reviews (Cochrane Reviews) and the Cochrane Database of Methodology Reviews (Methodology Reviews) up to April, 2005, and MEDLINE, PubMed, and PsycInfo from 1988 to the present. The keywords we used were “chronic fatigue syndrome” and “myalgic encephalomyelitis” in relation to epidemiology, aetiology, pathophysiology, diagnosis, definition, prognosis, prevention, and genetics. For the history of chronic fatigue syndrome, we searched the complete MEDLINE database and, when appropriate, publications from before 1988. In addition, we checked reference lists of articles identified by means of this search strategy and used relevant articles on these lists. We also used several book chapters and theses on chronic fatigue syndrome. ,FZXPSET $ISPOJDGBUJHVFp$ISPOJDGBUJHVFTZOESPNFp1TZDIPUIFSBQZp1TZDIPCJPMPHJDBMNPEFMp 6OTQFDJGJUZ 1TZDIPUIFSBQFVUr ] During the past two decades, there has been heated debate about chronic fatigue syndrome (CFS) among researchers, practitioners, and patients. Few illnesses have been discussed so extensively. The existence of the disorder has been questioned, its underlying pathophysiology debated, and an effective treatment opposed; patients’ organisations have participated in scientific discussions. In this review, we look back on several controversies over CFS with respect to its definition, diagnosis, pathophysiology, and treatment. We review issues of epidemiology and clinical manifestations, focusing on the scientific status of CFS. Modern neuroscience and genetics research offer interesting findings for new hypotheses on the aetiology and pathogenesis of the illness. We also discuss promising future issues, such as psychopathophysiology and mechanisms of improvement, and suggest multidisciplinary prospective studies of CFS and fatigue in the general population. These studies should pay particular attention to similarities to and differences from functional somatic syndromes and other fatiguing conditions. 346 whether the illness really exists.9 Researchers, practitioners, and patients have not been able to agree on the name (ME or CFS), on case definitions, on the acceptability of diagnosing CFS as an illness, on the absence of underlying pathophysiology and the need to continue research in somatic causes, or on the effectiveness of cognitive behaviour therapy (CBT). All these issues are discussed here, including those of epidemiology, clinical manifestations, and management of CFS. We also look forward to future studies resulting from a few promising hypotheses. Definitions The first studies of CFS were limited by the lack of proper diagnostic features and definitions. From 1988 onwards, several case definitions of CFS were developed.10–12 In 1994, a consensus was reached on a revised case definition from the US Centers for Disease Control and Prevention13 (panel). The importance of criteria on non-specific accompanying symptoms has been questioned, since the number of additional symptoms depends strongly on the assessment method used and no differences have been found in fatigue severity between patients whose disease met the criteria and those whose disease did not.14–16 The CFS definition was shown to lack specificity by comparison of groups of patients who met the case definition but had different symptom severities.17 Also, heterogeneity has been found within samples of patients with chronic fatigue.18 Between 2000 and 2002, international experts joined forces and identified ambiguities in the case definition for CFS. Guidelines for systematic and uniform case ascertainment and specific instruments for classification were developed to resolve ambiguities.19 In 2003, another case definition was proposed in an attempt to exclude psychiatric cases.20 Although they differ, all case definitions select severely fatigued groups of patients. Since CFS is neither a distinct nosological disorder nor a discrete diagnostic entity, the main purpose of a case definition is to identify patients who are at the tail end of the www.thelancet.com Vol 367 January 28, 2006