Bingold_Behandlung der Candidämie
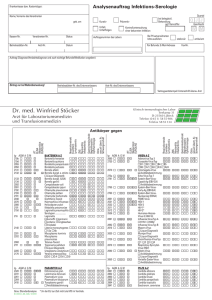
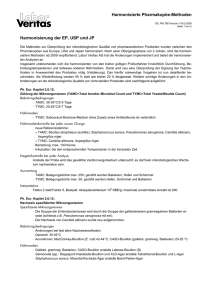
Werbung

Behandlung der Candidämie T. Bingold Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie Klinikum der Goethe Universität Frankfurt/ Main Behandlung der Candidämie • • • • Hintergrund/Medikation/Therapie IDSA 2009 PEG/DMYKG 2011 ESCMID 2012 Medical History Museum in Copenhagen 63 Jahre Intensivmedizin Candida Sepsis Kollef M et al. Clin Infect Dis. 2012;54:1739-1746 <24h >24h N = 224 Patienten zwischen 2002 und 2010 Letalität und Beginn der Antimykotika Therapie Arendrup Dan Med J 2013; 60(11): B4698 Invasive Pilzinfektionen auf ICUs Martin et al, NEJM 2003;348:1546-54 Epidemiology of Sepsis in USA 1979-2000 Candida spezies Candida glabrata 21% Candida albicans 63% Candida parapsilosis 5% Candida tropicalis 5% Candida krusei 2% Candida lusitaniae 1% Candida Candida kefyr dublinensis 1% 1% Candida norvegensis 0% Candida guilliermondii Candida 1% Candida sp. orthopsilosis 0% 0% Kresken M., Groll A. H., Lass-Florl C. und Korber-Irrgang B. fur die Studiengruppe Epidemiologie und Resistenzsituation bei Candida-Isolaten aus Blut und anderen primar sterilen Korperregionen gegenuber Antimykotika. Antiinfectives Intelligence, Rheinbach, 2013. Diagnostik Ullmann et al. 2012, CMI, 18 (Suppl. 7), 1–8 3 BK binnen 30 min Blutvolumen 40–60 ml (je 10 ml in je 3 aerobe und anaerobe Flaschen) Zeitgleich von unterschiedlichen Entnahmestellen (sterile Venenpunktion) Tägliche Abnahme von BK bei V.a. Candidämie Sensitivität 50–75% bei nicht neutropenen-, nicht vorbehandelten Patienten Candidämie im Internationalen Vergleich „Anamnese“ Arendrup Dan Med J 2013; 60(11): B4698 100 90 92 Prozent (%) 80 70 60 50 73 56 n >7000 Patienten 51 40 30 20 10 0 Europa und USA 33 25 24 16 1997-2011 19 9 5 2 30d Letalität 22-38% Therapieoptionen Falk Schuch , www:fotocommunity.de Wirkorte Abb. boundless-blog.ga Zell-Membran-Permeabilität Ergosterol Bindung Polyene Amphothericin B, Nystatin Cell-membrane-formation Inhibition der Ergosterol Produktion (Cytochrom P450) Azole Itraco-, Posaco-, Vorico-, ClotrimKetoconazol RNA und DNA Synthaseinhibition Pyrimidinanalog 5-Flucytosin Hemmung der Zellwandsynthese 1,3ß-Glucan Synthase Enzyme Echinocandine (Casop- Mica-, Anidulafungin) Pharmakokinetik Antimykotika Groll et al. Chemotherapie Journal 2011; 3: 67-93 In-vitro Empfindlichkeit nach CLSI Groll et al. Chemotherapie Journal 2011; 3: 67-93 Arendrup Dan Med J 2013; 60(11): B4698 Arendrup 2014 Curr Opin Infect Dis, 27:484–492 Proportion of invasive isolates with resistance Echinocandin resistance in Candida glabrata in Europe and America. Echinocandin Glucan Synthase Inhibitor FKS1p und 2p Mutation Arendrup 2014 Curr Opin Infect Dis, 27:484–492 Echinocandin Glucan Synthese Inhibitor Perlin, 2011 Future Microbiol. April ; 6(4): 441–457 Shields et al. Curr Opin Infect Dis 2015, 28:514–522 Erhöhte Rate an Therapieversagen von Echinocandinen bei invasiver C. glabrata Infektion: • Bei vorliegender FKS Mutation • Anamnestische Echinocandintherapie • GI Chirurgie binnen der letzten 30d • Caspofungin, Anidulafungin, Micafungin MIC >…. Indikation?? Prophylaxe Therapie mit BK Nachweis Candidämie Pre-emptive (Candidiasis ohne BK Nachweis) BK: Blutkultur Empirisch (Fieber) ESCMID guidelines 2012 Diagnosis and management of Candida diseases Cornely et al. 2012, CMI, 18 (Suppl. 7), 1–8 Antifungale Prophylaxe bei ITS Patienten Kürzlich chirurg. Eingriff und wiederholte gastrointestinale Perforationen Fluconazole 400mg/d SoR B, QoE I (Plazebo n=46) Kürzlich chirurgischer Eingriff und wiederholte gastrointestinale Perforationen Caspofungin 70/50mg/d SoR C, QoE II (single arm n=19) Kritisch kranke chirurg. Pat. mit erwartetem LOS ICU ≥ 3d; Fluconazol 400mg/d SoR C, QoE I (Plazebo n=260) Nach 48h Beatmung und erwarteter Beatmung über ≥ 72h Fluconazol 100mg SoR C QoE I (Plazebo, n = 104 +SDD) Beatmet, LOS Krkhs ≥3d, Antibiose, ZVK, und ≥ 1 von: PEN, RRT, Steroide, Immunsuppresion Caspofungin SoRC QoE II (Plazebo n=186) ESCMID guidelines 2012 Reccomendation on fever- and diagnosis driven therapy of candidaemia and invasive candidasis Cornely et al. 2012, CMI, 18 (Suppl. 7), 1–8 Antifungale Empirische Therapie Patienten mit Candida Isolaten aus BK, Antifungale Therapie; SoR A, QoE II ITS Patienten mit persistierendem Fieber ohne Hinweis auf bakterielle Ursache (Reduktion der Letalität) Fluconazole oder Echinocandine; SoR C; QoE II ITS Patienten mit positivem 1,3 ß-D-Glucan Test Alle Antimykotika; SoR C, QoE II ITS Patienten mit Fieber unter Breitbandantibiose und APACHE II 16 Fluconazol 800mg; SoR D QoE I ITS Patienten mit Candida Isolaten aus dem respiratorischen Sekret; Alle Antimykotika; SoR D QoE II Empirische Therapie non–critically ill, non- immunosuppressed patients high prevalence Fluconazole-resistant C. glabrata (>10%) Echinocandin Eschenauer et al. 2015 Annals of Pharmacotherapy vol. 49 no. 9 1068-1074 Abfall von ROS Produktion durch Alveolar Macrophagen bei Besiedlung mit C. albicans Roux et al. 2009 Crit Care Med 37:1062–1067 ROS: Reactice Oxygene Species Algorithmus zur Initialtherapie bei Candidämie Pappas PG et al. Clin Infect Dis 2009; 48:503-35. Patient weniger kritisch krank * Patient schwerer bis kritisch krank * Azol-Vorexposition* nein ja C. glabrata/krusei bis Resistogramm vorliegt nein C. parapsilosis ja Echinocandin * Fluconazol Unzureichendes Ansprechen * ja Leberdysfunktion oder interaktionsträchtige Komedikation ? nein Deeskalation möglich ? Alternativ Einsatz von Ampho B möglich Ggf. kein Caspofungin Anidulafungin, Caspofungin, Micafungin Diagnosis and management of Candida diseases ESCMID guidelines 2012 Cornely et al. 2012, CMI, 18 (Suppl. 7), 1–8 Dauer der Therapie Candidämie ohne Organbeteiligung • 14d Therapie nach letzter positiver BK Dauer Kontrolle DeEskalation • • • • 1 BK / Tag bis BK negativ [B] TEE [B] Augenhintergrundkontrolle [B] Thromboskontrolle bei liegenden i.v. Kathetern [B] • De-Eskalation auf Fluconazole nach 10 d von i.v. auf p.o. wenn möglich und sensibel Reccomendation for candida meningitis ESCMID guidelines 2012 Cornely et al. 2012, CMI, 18 (Suppl. 7), 1–8 Candida Meningitis Therapie Liposomales Ampho. B 3mg/kg für 10 Wochen + Flucytosine 150mg/kg für 10 Wochen, im Anschluss Fluconazole 3mg/kg für 5 Wochen ; SoR B, QoE III Liposomales Ampho. B 3mg/kg für 4 Wochen + Fluconazole 6mg/kg für 4 Wochen ; SoR B, QoE III Voriconazol 12/6 mg/kg SoR C, QoE III, Therapeutic drug monitoring recommended Fluconazol 800mg; SoR C QoE III Caspofungin 70/50 mg für 4 Wochen, im Anschluss Fluconazol 400 mg für 2 Wochen SoR D QoE III QoE III: Evidenz from opinions of respected authorities, based on clinical experiences, descriptive case studies Reccomendation for candida endocarditis ESCMID guidelines 2012 Cornely et al. 2012, CMI, 18 (Suppl. 7), 1–8 Candida Endocarditis Therapie Native Klappe, Operation binnen einer Woche; SoR A, QoE II Liposomales Ampho B ± Flucytosin für 6-8 Wochen, im Anschluss Fluconazol SOR B QoE II Oder Caspofungin ± Flucytosin; SOR C QoE II Prothetische Klappe, Operation binnen Tagen SoR A QoE III Prothetische Klappe, falls keine Operation möglich Liposomales Ampho B 5mg/kg Caspofungin 70/50 mg SoR B QoE III Lebenslang Fluconazol 400-800mg SoR C QoE III Zusammenfassung Herzlichen Dank für Ihre Aufmerksamkeit [email protected]