ASCO 2012: N dj t N W d Neoadjuvant, Neue Wege und Beiträge
Werbung

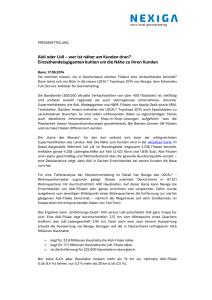
Campus Innenstadt | Campus Großhadern Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012: N Neoadjuvant, dj t N Neue W Wege und d Beiträge aus München Prof. Dr. Nadia Harbeck Brustzentrum der Universität München Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe Ludwig-Maximilians-Universität München Direktor: Prof. Dr. Klaus Friese ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 2 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 3 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck ASCO 2012: Mammakarzinom Neoadjuvant: HER2 positiv: duale Blockade neue Therapiekonzepte Adjuvant: Bisphosphonate – Benefit begrenzt auf Subgruppen Chemotherapie: zusätzliche Substanzen nicht sinnvoll, Taxane bei pN0 wirksam Metastasiert: HER2 positiv: TDM1 – practice changing data (EMILIA Studie) vielversprechende neue Therapeutika … KLINIKUM DER UNIVERSITÄT MÜNCHEN® 4 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck NSABP B-41: B 41: neoadjuvante anti-HER2 Therapie Robidoux A et al. al ASCO 2012 Abst #506 KLINIKUM DER UNIVERSITÄT MÜNCHEN® 5 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck NSABP B-41: B 41: neoadjuvante anti-HER2 Therapie Robidoux A et al. ASCO 2012 Abst #506 KLINIKUM DER UNIVERSITÄT MÜNCHEN® 6 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe KLINIKUM DER UNIVERSITÄT MÜNCHEN® Brustzentrum Klinik und Poliklinik für Frauenheilkunde Baselgaund et Geburtshilfe al, SABCS 20 1.0 1.0 0.8 0.8 OS S estimate DFS estimate TECHNO: pCR is a prognostic factor for both DFS and OS in HER2-positive eBC 0.6 pCR 0.4 0.6 pCR 0.4 No pCR 0.2 No pCR 0.2 Log-rank p=0.0033 Log-rank p=0.0074 0 0 0 6 12 18 24 30 36 42 48 54 60 0 6 12 18 24 30 36 42 48 54 60 Time (months) No. at risk pCR 84 no pCR 133 79 118 61 86 57 76 43 56 Time (months) 16 27 5 10 No. at risk pCR 84 no pCR 133 79 118 62 96 62 84 47 65 17 33 7 14 Untch, et al. JCO 2011 Subtype-specific general adj adjuvant ant strategies © AGO e. V. in der DGGG e.V. sowie in der DKG e.V. Guidelines Breast Version 2012.1D www.ago-online.de HR+/HER2- and „low risk“: •endocrine therapy without chemotherapy ++ HR+/HER2- and „high risk“: •Conventionally dosed AT-based chemotherapy •Dose dense & escalated in case of high tumor burden Followed by endocrine therapy ++ + ++ HER2+ C Consider id neoadjuvant dj t approach h Trastuzumab plus • Sequential A/T-based regimen with concurrent T+H • Anthracycline-free, Anthracycline free carboplatin carboplatin-cont. cont regimen • Dose dense & escalated in case of high tumor burden + ++ ++ + + TNBC •Consider neoadjuvant approach •Conventionally dosed AT-based chemotherapy Dose dense & escalated •Dose •Carboplatin + ++ + +/-* *only within clinical trials T DM1 T-DM1 Seite 10 <22..01.11> | <BKK 2011> | <Prof. N. Harbeck> ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 11 22.07.2012 Chau et al, ASCO 2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 12 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 13 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe Post-treatment Ki-67 and patient outcome von Minckwitz et al, ASCO 2012 ADAPT: Dynamic Test System Dowsett et al, 2007, Piccart 2009 22.07.2012 WSG GmbH 15 ADAPT – Studie • HR+: Vermeidung von Übertherapie • HER2+/TN: Neue Substanzen, Substanzen Surrogatmarker für pCR Wirksam‐ keit Prognose B I o P S IE* HR + Therapie 3 Wo HER2 + TN RS Proliferation Apoptose 22.07.2012 B I o P S IE* Niedrigrisiko oder gutes Ansprechen gutes Ansprechen Endokrine Therapie allein HR+ HER2+ Frühe Surrogatmarker für TN RS Proliferation Apoptosis WSG GmbH Hochrisiko oder Hochrisiko oder schlechtes Ansprechen CT ÆEndokrine Therapie pCR Vielversprechende, zielgerichteteTherapien (TDM1, Pertuzumab, …) 16 ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 17 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck ASCO 2012: was bleibt praxisrelevant beim frühen Mammakarzinom ? Neoadjuvant: HER2 positiv: Höchste pCR Raten durch duale Blockade TDM1 keine TDM1: k i kardialen k di l Si Sicherheitsbedenken h h it b d k Frühe Evaluation des Ansprechens wichtig für Patientin: Neues: Erste Studie zum NGS beim Mammakarzinom Ki-67 Abfall, aber auch Klinik, Bildgebung … Pathways zur weiteren Analyse, wenig drug targets … … KLINIKUM DER UNIVERSITÄT MÜNCHEN® 18 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe Prognostic impact of local surgical treatment of the primary tumor in metastatic breast cancer I. Himsl°, N. Ditsch°, M. Lenhard°, J. Engel¹, M. Untch², I. Bauerfeind³, K. Friese°, N. Harbeck°, S. Kahlert° #96160 °Dept. OB/GYN Grosshadern and ¹Institute for Biostatistics and Epidemiology, Ludwig Maximilians University Munich, ²Helios Klinikum Berlin-Buch, ³Klinikum Landshut, Germany Introduction: MBC is an incurable disease and the treatment aims are palliative. Still local therapy is associated with improved survival in several studies. It is not known whether the difference in OS is the result of a selection bias or caused by dissemination of tumor stem cells in pat. without surgery. Method: Mono-institutional retrospective review from 1990-2006 to identify the impact of surgical therapy of the primary tumor. Results: We identified 269 pts. with primary MBC, 63 of whom had received no surgical local treatment. Mean follow up is 65 m for pts., observed mortality 87%. Location of metastases were bone only (36%), visceral or soft tissue (one organ only, 19%), multiple organs (40%) and including CNS metastases (5%). 50% had G3 tumors, 25% negative receptor status, 7% non-resectable local disease and 57% symptomatic metastases. In univariate analysis, pat. without local treatment had a median OS of 14.4m, pts. with local therapy 28.1m (p<0.001). Pts. not receiving local treatment were significantly more likely to have multiorgan or CNS involvement (p< 0.001), symptoms t att diagnosis di i ((p=0.009), 0 009) non-resectable t bl ttumor ((p<0.001) <0 001) and were more likely to die within the first 30d after diagnosis (p< 0.001). In multivariate analysis, local treatment had no significant impact on OS. The only significant variables were: number of involved organs, symptoms at diagnosis, receptor status, grading, and size of the local tumor. The effect of local treatment on OS was not homogenous across subgroups. Local treatment was a significant factor in tumors with only one involved organ or asymptomatic disease disease. In more advanced disease groups groups, local treatment did not result in a significant OS benefit. n T1-3 158 w/o local tx. with local tx. with local therapy with local therapy w/o local therapy with local therapy w/o local therapy Mean OS 17.3 vs. 38.8 months p < 0.001 w/o local therapy Mean OS 10.5 vs. 20.4 months p = n.s. RR with local therapy with local therapy w/o local therapy w/o local therapy Mean OS 28.6 vs. 16.2 months p = n.s. Kaplan MeierEstimate: surgery vs no surgery & OS Mean OS 4.0 vs. 5.5 months p = n.s. Number of met. organ systems and OS 92 21 (23%) 71 (77%) T4 not res. 19 16 (84%) 95%-CI p-value T1-3 w/o local therapy 3 (16%) p < 0.001 G1,2 135 42 (31%) 93 (69%) G3 134 21 (16%) 113 (84%) p = 0.003 ER/PR pos. 202 51 (25%) 151 (75%) ER/PR neg. 67 1 organ 148 20 (14%) 128 (86%) 2 organs 59 11 (17%) 48 (83%) 3 organs 38 14 (37%) 24 (63%) >3 organs 24 bone only 98 sing. visc./soft multiple + cns no sympt.116 T4 resect. vs. T1-3 1.3 1.0 – 1.7 p = 0.071 T4 nott res. vs. T1-3 26 2.6 1 5 – 4.7 1.5 47 p = 0.001 0 001 G3 vs. G1-2 12 (18%) 55 (82%) p = n.s. 1.3 1.0 – 1.8 1.2 – 2.3 Mean OS 13.3 vs. 37.2 months p < 0.001 p = 0.037 ER/PR neg. vs. pos. 1.7 p = 0.001 2 organs inv. vs. One only 1.6 1.2 – 2.3 p = 0.004 3 organs inv. vs. One only 2.0 1.4 – 3.0 p = 0.001 >3 organs vs. One only 3.0 6 (25%) 18 (75%) p < 0.001 12 (12%) 86 (88%) 51 8 (16%) 43 (84%) 108 37 (34%) 71 (66%) 12 6 (50%) 153 death w/i 30 days 13 All 296 45 (29%) 108 (71%) 5 (38%) with local therapy p = 0.01 p = 0.009 8 (62%) p = 0.003 63 (21%) 233 (79%) Pts. demographics T4 resectable p = n.s. T4 not res. p = n.s. G1,2 p < 0.001 G3 p = 0.002 ER/PR pos. p < 0.001 ER/PR neg. p = 0.022 1 organ p < 0.001 2 organs p = n.s. 3 organs p = n.s. >3 organs p = n.s. bone only p = 0.01 sing. visceral/soft p = 0.017 w/o local therapy Mean OS 18.4 vs. 23.0 months p = n.s. 6 (50%) p < 0.001 18 (16%) 98 (84%) symptoms w/o local therapy Mean OS 14.4 vs. 18.3 months p = n.s. 1.8 – 5.2 p = 0.001 Not significant: local treatment, age < 40 and type of o metastases etastases multivariate analysis OS 0.1 Symptomatic disease and OS multiple p = n.s. + cns p = n.s. no sympt. p < 0.001 symptoms p = n.s. all p < 0.001 0.2 0.4 no surgery better 1 10 2 4 surgery better Subgroup analysis (values above 1 if with therapy is superior) with local therapy with local therapy w/o local therapy Mean OS 13.4 vs. 27.9 months p = 0.005 w/o local therapy Mean OS 3.5 vs. 2.1 months p = n.s. Localisation of metastases and OS with local therapy T4 resectable with local therapy w/o local therapy Mean OS 14.4 vs. 28.1 months p < 0.001 p-value 26 (16%) 132 (84%) with local therapy Mean OS 21.9 vs. 41.6 months p = 0.003 Conclusion: Consistent with other studies, our cohort showed significantly improved OS in univariate analysis if the breast primary tumor had been removed in metastatic disease. Yet, the decision for local treatment was biased by the extent and presentation of metastatic disease. Pts. with more advanced MBC seem not to benefit from removal of the primary tumor. However, we see significant influence in pts. with limited and asymptomatic MBC. The potential dissemination of tumor stem cells from the breast primary in metastatic but locally untreated disease may influence prognosis in pts. with limited disease only. References: Impact of breast surgery on survival in women presenting with metastatic breast cancer. Pathy NB et al. Br J Surg. (2011) Removal of primary tumor improves survival in metastatic breast cancer. Does timing of surgery influence outcomes? Pérez-Fidalgo JA et al. Breast. (2011) Local-regional radiotherapy and surgery is associated with a significant survival advantage in metastatic breast cancer patients patients. Ly BH et al. al Tumori. Tumori (2010) ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 20 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 21 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 22 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe SUCCESS B STUDIE Multizentrische Phase III-Studie Vergleich: 3x FEC Æ 3x Doc vs. 3x FEC Æ 3x DG Primäres Mammakarzinom; N+ oder high risk N0; HER2- positiv n=793 793 CTC‐Analyse und HER2 Phänotypisierung mittels CellSearch System CTC-Detektion mittels CellSearch System: HER2 - Phänotypisierung: Blutabnahme vor Beginn der adjuvanten Anti-CK-Fluorescein Isothiocyanate Chemotherapie (FITC) Immunomagnetische Anreicherung durch Klassifizierung der Färbung: Antikörper gegen Epcam Fluorescent anti-Cytokeratin Antikörper (CK8,18,19–phycoerythrin) Anti-CD45 Antikörper (CD45– allophycocyan) negativ ((-)) schwache (+) mäßige (++) starke (+++) Cut-off: 1 >/=CTC,, >/=1 CTC Her2+++ KLINIKUM DER UNIVERSITÄT MÜNCHEN® 23 Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe – Campus Innenstadt 300 Ergebnisse 638 Blutproben vor adjuvanter Chemotherapie CTC positiv 40 40,2% 2% (n=257) (n 257) Median 4,52; Range 1-1689 CTC pos, Her2 pos 250 CTC pos, Her2 neg 200 150 100 50 0 total 1 2 3 4 >/=5 CTC HER2-Status auf CTCs (Prozent der CTC-positiven Patienten) Negativ: Schwach: Mäßig: Stark: 12,5% (n=32) 8,9% (n=23) 21,4% 21 4% (n=55) 57,2% (n=147) CTC pos, Her2CTC pos, Her2+ CTC pos, Her2++ CTC pos, Her2+++ CTC neg g Keine Korrelation mit Tumorgröße Grading HR-Status: ER PR y p Lymphknotenbefall (p=0,347) (p=0,643) (p 0,643) (p=0,597) (p=0,194) (p , ) (p=0,808) KLINIKUM DER UNIVERSITÄT MÜNCHEN® 24 Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe – Campus Innenstadt KLINIKUM DER UNIVERSITÄT MÜNCHEN® Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe ASCO 2012 | Prof. Harbeck KLINIKUM DER UNIVERSITÄT MÜNCHEN® 26 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe EVIDENZBASIERTE BRUSTKREBS-THERAPIE Jährlich aktualisierte, evidenzbasierte Empfehlungen zur Diagnostik und Therapie AGO (DKG, DGGG) www.ago-online.de www.karger.com/brc KLINIKUM DER UNIVERSITÄT MÜNCHEN® 27 22.07.2012 Brustzentrum Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe