Management von Durchbruchinfektionen
Werbung

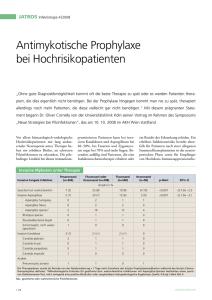
Management von Durchbruchinfektionen Helmut Ostermann und Christina Rieger Klinisches Beispiel Teil 1 Pat. B. S., männlich, 68 Jahre, AML M2 (Erstdiagnose) Induktions-CTx mit Cytarabin/ Mitoxantron (“s-HAM”) FUO in Zytopenie, empirische Antibiose mit Piperacillin/ Tazobactam nicht wirksam HR-CT: V. a. Invasive Pilzerkrankung der Lunge • Therapie mit liposomalem Amphotericin B Æ klinische Besserung, Regeneration der Leukozyten, Knochenmarkaspirat nach Induktion Blastenfreiheit Æ Plan: Fortführung der CTx unter Pilz-Prophylaxe mit Posaconazol 2 im Klinisches Beispiel Teil 2 Konsolidierungs-CTx mit Cytarabin/ Daunorubicin/ Thioguanin (“TAD”) antimykotische Prophylaxe mit Posaconazol (3 x tgl. 200 mg p.o.) erneut FUO in Zytopenie, empirische Antibiose mit Breitspektrum Penicillin nicht wirksam, Umsetzung der Antibiose auf Vancomycin/ Meropenem positive BK: Klebsiella pneumoniae (auf Meropenem gut empfindlich) deutliche klinische Verschlechterung des Patienten HR-CT: Residuen der Pilzpneumonie, sonst o. p. B. 3 Klinisches Beispiel Teil 3 Ursache der Infektion? Mikrobiologische Diagnostik erbringt Nachweis: Trichosporon asahii mehrfach in Blutkultur nachweisbar Æ Resistenz gegen Fluconazol und Caspofungin, Amphotericin B- und Voriconazolempfindlich keine Resistenztestung für Posaconazol verfügbar Æ bei Hochrisiko-Situation: Umsetzung der Antimykose auf Kombination von liposomalem Amphotericin B und Voriconazol Ö Nach 3 Tagen deutliche Verbesserung des klinischen Status des Patienten Ö Fortsetzung der Kombinationstherapie bis zur Leukozytenregeneration, danach Maintainance mit Voriconzol Ö Pat. seither in kompletter Remission der AML, keine weiteren Infekte 4 Was ist eine Durchbruchinfektion Durchbruchinfektionen in klinischen Studien –Prophylaxe –Empirische Therapie –Therapie der IFI Ursachen für Durchbruchinfektionen – Wirkspektrum – Dosierung – Resorption – Interaktion Was tun bei Durchbruchinfektionen Durchbruchinfektion = Therapieversagen Prophylaxe Empirische Therapie Was ist eine Durchbruchinfektion? Prophylaxe – Proven oder Probable IFI – Empirische Behandlung mit Antimykotika ? – Besiedlung ? Empirische Therapie – Proven oder Probable IFI – Umsetzen der Antimykotika ? – Besiedlung ? Was ist eine Durchbruchinfektion? Prophylaxe Posaconazol Cornely: – ... incidence of proven or probable invasive fungal infection during the treatment phase, as adjudicated by an expert panel whose members were unaware of the treatment assignments, according to consensus criteria of the European Organisation for the Research and Treatment of Cancer and the Mycoses Study Group Micafungin van Bourik –... criteria for proven and probable infection are consistent with those for invasive fungal infection described by the Invasive Fungal Infections Cooperative Group of the European Organization for Research and Treatment of Cancer, National Institute of Allergy and Infectious Diseases Mycoses Study Group.... Fungal infection was defined as suspected if fevers (temperature, 38C [100.4F]) persisted for 196 h during the neutropenic phase, despite broad-spectrum antibacterial therapy, and led to the initiation of empirical antifungal therapy Micafungin - Hiramatsu –... proven or probable infection according to the Invasive Fungal Infections Cooperative Group of the European Organization for Research and Treatment of Cancer, the National Institute of Allergy, and the Infectious Diseases Mycoses Study Group [12]. Fungal infection was defined as suspected if fevers (temperature C38C [C100.4F]) persisted for [96 h during the neutropenic phase, despite broad-spectrum antibacterial therapy and led to the initiation of empirical antifungal therapy Was ist eine Durchbruchinfektion? Prophylaxe Posaconazol Cornely: – Primary analysis ... incidence of proven or probable invasive fungal infection during the treatment phase, – Secondary analysis ... incidence of invasive aspergillosis, the incidence of invasive fungal infection within 100 days after randomization Micafungin van Bourik –.... absence of proven, probable, or suspected systemic fungal infection through the end of prophylaxis therapy and as the absence of a proven or probable systemic fungal infection through the end of the 4-week posttreatment period Micafungin – Hiramatsu – .... absence of proven, probable, or suspected systemic fungal infection through the end of prophylaxis therapy and as the absence of a proven or probable systemic fungal infection through the end of the 4-week posttreatment period Durchbruchinfektionen in Prophylaxestudien Proven & Probable POS / MICA FLU / ITRA Possible POS / MICA FLU / ITRA Cornely 2,3 % 8,3 % 26,6 % 37,6 % Van Bourik 1,6 % 2,4 % 15,1 % 23,0 % Hiramatsu 2,0 % 2,0 % 4,0 % 12,0 % Durchbruchinfektionen in Empiriestudien Proven & Probable AmB Vori Caspo Ambisome Walsh 1999 7,8 % 3,2 % Walsh 2002 1,9 % 5,0 % Walsh 2004 5,2 % 4,4 % Kolonisation vs Infektion Candida Score – Leon CID 2009 total parenteral nutrition x 1 plus surgery x 1 plus multifocal Candida colonization x 1 plus severe sepsis x 2 Cut off ≥ 3 Candida Score – Leon et al -- Crit Care Med 2009 Was bedeutet Therapieversagen? Persistierender Nachweis von Candida in der Blutkultur Auftreten neuer Pilzherde Progress der pulmonalen Infiltrate? Verschlechterung des Allgemeinzustands des Patienten? In-Vitro-Aktivität antimykotischer Substanzen A. fumigatus (n=26) A. terreus (n=20) A. flavus (n=16) A. niger (n=8) Rhizomucor spp. (n=7) Absidia spp. (n=13) Rhizopus spp. (n=12) Mucor spp. (n=14) Penicillium spp.(n=7) M IC (µg/m l) 90% results against all tested species. Strains showing M ICs > 8 μg/m l for azoles (incl. CAS) and M ICs > 4 μg/m l for AM B form ulations were designed as resistant (>8), M ICs coded =8 or <8 represent interm ediate or susceptible species, respectively. AM B 1 4 2 2 1 1 2 1 1 l-AM B 2 4 2 2 0.5 2 2 0.25 0.25 CAS* 0.5 0.5 1 0.5 >8 >8 >8 >8 >8 ITZ 2 2 1 4 >8 >8 >8 >8 >8 VRZ 0.5 0.5 1 1 >8 >8 >8 >8 >8 PO S 0.5 0,5 0.5 0.5 4 1 4 8 2 Lass-Flörl C. et al., ICAAC 2007, Poster #543 16 Versagen bei primärer Resistenz Candida krusei – Fluconazol Amphotericin B – Aspergillus terreus Zygomyceten - Voriconazol Therapieversagen - Sind Medikamentenspiegel notwendig? Therapieversagen durch niedrige Medikamentenspiegel? Pascual et al CID 2008 Therapieversagen durch niedrige Medikamentenspiegel? Pascual et al CID 2008 Größenzunahme von Aspergillusherden im CT unter Therapie Caillot JCO 2001 IRIS – Immune reconstitution inflammatory syndrom Miceli, Cancer 2007 19 Patienten mit hämatologischer Neoplasie Mit Erholung der Neutrophilen – Verschlechterung der pulmonalen Funktion – Verschlechterung der radiologischen Befunde – Absinken des Serum Galaktomannans Durchbruchinfektionen - Diagnostik Wann Diagnostik ? –Surveillance ? – bei Fieber ? – Bei anderen klinischen Zeichen ? Welche – Serologie / PCR? – Abstriche / Kulturen? – Rö Thorax / CT ? Durchbruchinfektionen Therapie Klassenwechsel - Kombination Therapie der Durchbruchinfektion in der Prophylaxe Wechsel der Substanzklasse Azol Æ Polyen oder Echinocandin Polyen Æ Azol oder Echinocandin Echinocandin Æ Azol oder Polyen Aber falls nur „empirische Durchbruchinfektion“ Æ keine Änderung ? Therapie der Durchbruchinfektion in der Empirie Wechsel der Substanzklasse Azol Æ Polyen oder Echinocandin Polyen Æ Azol oder Echinocandin Echinocandin Æ Azol oder Polyen Management von Durchbruchinfektionen in der Prophylaxe Prophylaxe Antibiotikarefraktäres Fieber Fortsetzen der Prophylaxe Klassenwechsel Management von Durchbruchinfektionen in der Prophylaxe Prophylaxe Proven / Probable IFI Klassenwechsel Management von Durchbruchinfektionen in der Empirie Empirische Therapie Antibiotikarefraktäres Fieber Possible IFI Fortsetzen der Empirie Klassenwechsel Management von Durchbruchinfektionen in der Empirie Empirische Therapie Proven / Probable IFI Klassenwechsel Management von Durchbruchinfektionen bei IFI Therapie der IFI Progress der IFI Immunrekonstitution ? Ja Keine Änderung Nein Klassenwechsel Kombinationstherapie bei Durchbruchinfektionen? Möglichst innerhalb klinischer Studien ! Antimykotische Kombinationstherapie Offene Fragen der Kombinationstherapie: Klinischer Synergismus? Additive Effekte? Indifferenz? Klinischer Antagonismus? Höhere Ansprechraten? Schnelleres Ansprechen? Kürzere Behandlungsdauer? Kürzere Hospitalisation? Verringerte Morbidität / Mortalität? Management von Durchbruchinfektionen - Fazit Bei Verdacht auf Durchbruchinfektion Æ Diagnose sichern Wirksamkeit der antimykotischen Therapie gegeben? – Erreger ? – Wirkspiegel ? Alternativen zur Durchbruchinfektion beachten ! – Immunrekonstitution –Kolonisierung vs Infektion Klassenwechsel vor Kombinationstherapie