1,4 MB
Werbung

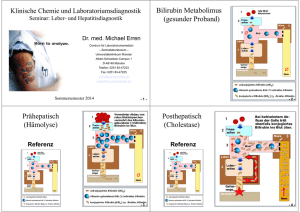
Klinische Chemie und Laboratoriumsdiagnostik Seminar: Leber-, Pankreas- und Hepatitisdiagnostik Dr. med. Michael Erren Centrum für Laboratoriumsmedizin – Zentrallaboratorium – Universitätsklinikum Münster Albert-Schweitzer-Campus 1 D-48149 Münster Tel.: 0251 83-47233 Fax: 0251 83-47225 [email protected] www.klichi.uni-muenster.de Sommersemester 2017 Akute Virushepatitis: Klinik Asymptomatisch (70%), insbesondere Kinder und Hepatitis C Inkubationszeit: 3 - 4 Wochen Prodromalstadium (1 Woche) – Grippale Symptome – Gastrointestinale Beschwerden – Ev. Milz- / Lymphknotenvergrößerung – Ev. Athralgien / Exanthem (HBV 10%) Organmanifestation (4 - 8 Wochen) – Häufig Lebervergrößerung – Ikterischer (30%) bzw. cholestatischer Verlauf (5%) (Ikterus, Puritus, Stuhl, Urin) Bilirubin Metabolimus (gesunder Proband) Prähepatischer Ikterus (Hämolyse) Referenz Prähepatischer Ikterus (Hämolyse) Hämolyse-Zeichen: • Plasma / Serum lachsfarben • LDH ↑ • K+ ↑ • Ery ↓ • Hb ↓ • fHb ↑ • Haptoglobin ↓ • Hämopexin ↓ • Retikulozyten ↑ • Blut: indirektes Bilirubin ↑↑, direktes Bilirubin Ø • Stuhl: dunkel (Sterkobilinogen ↑) • Harn: Bilirubin Ø, Urobilinogen ↑ (cave: Proteinurie) Posthepatischer Ikterus (Cholestase) Referenz Posthepatischer Ikterus (Cholestase) Cholestase posthepatisch: • Blut: ‐ direktes Bilirubin ↑ ↑ ↑ ‐ indirektes Bilirubin Ø • Blut: AP ↑↑ ↑, ‐GT ↑ • Stuhl: entfärbt (Sterkobilinogen Ø) • Harn: dunkel (direktes Bilirubin ↑, Urobilinogen Ø) Intrahepatischer Ikterus (z.B. Hepatitis) Referenz Intrahepatischer Ikterus (z.B. Hepatitis) Cholestase intrahepatisch: • Blut: ‐ direktes Bilirubin ↑↑ ‐ evtl. indirektes Bilirubin ↑ • Blut: GPT ↑, GOT ↑ (AP ↑, ‐GT ↑) • Stuhl: leicht entfärbt (Sterkobilinogen reduziert) • Harn: dunkel (direktes Bilirubin ↑, Urobilinogen ↑) Bilirubin im Serum Ikterus Pathophysiologie Gesamt Bilirubin Indirektes Bilirubin Direktes Bilirubin Erkrankung Prähepatisch Glukuronidierungskapazität unzureichend Hämolytische Anämie (Haptoglobin, Retikulozyten) Hepatisch Bilirubinverwertungsstörung Hepatitis (GPT, GOT) Posthepatisch Abflußbehinderung des direkten Bilirubins Cholestase (-GT, AP) Bilirubin und Urobilinogen Bili Urin im Urin Ikterus Bilirubin Urobilinogen Prähepatisch Hepatisch Posthepatisch Zelluläre Topograhie Zellulärer Enzyme • Zytoplasma: GPT, GOT (30%), LDH5 • Mitochondrien: GOT (70%), GLDH • Membrangebunden: AP, -GT, (LAP) GLDH Sekretionsenzyme • PCHE • Albumin, Präalbumin • Gerinnungsfaktoren: Protrombinkomplex, Faktor V Labor • Akut: GPT > GOT (500 - 3.000 U/l; De Ritis: GOT / GPT< 1) Chron.: GOT > GOT (50 -100 U/l; De Ritis: GOT / GPT > 1) • Serum: Bilirubin ↑; Urin: Bilirubin ↑ + Urobilinogen ↑ • Ev. AP ↑, γ-GT ↑ • Serumeisen ↑, Kupfer ↑, γ-Globuline ↑ (IgG) • Ev. Lymphozyten ↑ • Ev. Eiweißelektrophorese, BSG ↑, CRP ↑ • Leberinsuffizienz: PCHE ↓, Quick ↓, Albumin ↓ • Serologie: IgG alt (Immunstatus) IgM frisch oder HBV-Reaktivierung • Viruslast Akute Hepatitis I Akute Hepatitis II Pankreasdiagnostik • Lipase akut: >3x (50 - 100x), chronisch: häufig nicht erhöht • Amylase (auch Urin), Pankreas-Isoamylase • CRP, Leukozyten, LDH • -GT, AP, direktes Bilirubin (Obstruktion) • Triglyceride, Calcium (Ätiologie, Prognose), Parathormon • Glucose, Insulin, C-Peptid • CA 19-9 Funktionsteste: Direkt: • (Sekretin-Pankreozymin-Test; zu aufwendig) Indirekt: • (Flurescein-Dilaurat-Test; Problem: Darm-Malabsorption, Leber- und Niereninsuffizienz) • Chymotrypsin (Präparate absetzen) oder Elastase 1 im Stuhl Bakteriologische, zytologische Diagnostik: • Feinnadelpunktion unter Sonokontrolle Virushepatitis Genom Übertragungsweg A B C RNA DNA zytopathisch fäkal-oral Fulminant 0,2% - 3% D E Italien Afrika/Asien RNA RNA RNA immunologisch zytopathisch zytopathisch zytopathisch parenteral parenteral parenteral fäkal-oral sexuell (sexuell) perinatal perinatal 1% selten (TierReservoir) >2% 3% (10%) (10%) (20%) Chronisch, Zirrhose, Karzinom nein ja ja!!! ja nein Impfung aktiv/passiv ja/ja ja/ja nein/nein (nein/nein) ja/nein Antivirale Therapie (akut/chronisch) nein ja ja - nein Hepatitis A: Diagnostische Marker Marker Definition Bedeutung Anti-HAV-total (Blut) Antikörper gegen HAV (IgG + IgM) Durchseuchungsmarker => Immunität Anti-HAV-IgM (Blut) Antikörper gegen HAV (IgM) frische Infektion RNA des HAV direkter Virusmarker, beweist akute Infektion HAV-RNA (Stuhl) HA-Ag HAV-Antigen (Stuhl) (Antigen der Virusoberfläche) Infektiösitätsmarker Hepatitis A: serologischer Verlauf A Kinetik Hepatitis B: Schematischer Aufbau Marker HBV Definition Bedeutung Hepatitis B:Virus-DNA Diagnostischedirekter Marker Virusnachweis HBV-DNA HBsAg Oberflächenprotein akute/chronische Infektion, frühester Marker, Infektiösität HBeAg ins Blut sezerniertes Virusprotein (teilweise identisch mit HBcAg) Infektionsmarker: hohe Infektiösität Anti-HBc Antikörper gegen HBcAg (IgG + IgM) Früh- und Durchseuchungsmarker, lebenslang positiv nach HBVKontakt (akute/chronische, abgelaufende Hep.-B) Anti-HBc-IgM Antikörper gegen HBcAg (IgM) hohe Titer beweisen akute Hep.-B-Infektion Anti-HBe Antikörper gegen HBeAg löst HBeAg ab; spricht für geringere/fehlende Infektiösität Anti-HBs Antikörper gegen HBsAg abgelaufende Hep.-B (in Verbindung mir Anti-HBc); Immunität (einziger Antikörper nach Hepatitis-B-Impfung) isolierter Anti-HBc-Status isolierter Anti-HBs-Status Reaktivierung Hepatitis B akut: serologischer Verlauf Hepatitis D • Hepatitis Delta Virus • inkomplettes („nacktes“) Virus (Viroid), benötigt für Replikation Hülle des HBV (HBsAg) Hepatitis D Virus (HDV) korrespondierende Antikörper Hülle: HBsAg (Leih-Ag) anti-HBs Kern: HDV-Ag anti-HDV Kern: HDV-RNA Simultan-Infektion : HBV + HDV (Heilung 90%) Super-Infektion : HBsAg-Trägers (häufiger, fulminant / chronisch) Klinische Chemie und Laboratoriumsdiagnostik S i Seminar: LeberL b undd Hepatitisdiagnostik H titi di tik Bilirubin Metabolimus ( (gesunder d Proband) P b d) Dr. med. Michael Erren Centrum für Laboratoriumsmedizin – Zentrallaboratorium – Universitätsklinikum Münster Albert-Schweitzer-Campus 1 D-48149 Münster Telefon: 0251 83-47233 Fax: 0251 83-47225 erren@uni-muenster erren@uni muenster.de de www.klichi.uni-muenster.de Sommersemester 2017 -1- -2- Prähepatisch (Hä l ) (Hämolyse) Posthepatisch (Ch l (Cholestase) ) Referenz Referenz -3- -4- Intrahepatisch ( B H (z.B. Hepatitis) ii ) Zelluläre Topograhie Zellulärer Enzyme Referenz • Zytoplama: GPT, GOT (30%), LDH5 • Mitochondrien: GOT (70%), GLDH • Membrangebunden: AP, -GT, (LAP) GLDH S k ti Sekretionsenzyme • PCHE • Gerinnungsfaktoren: Protrombinkomplex, Faktor V • Albumin, Präalbumin -5- -6- -7- -8- Hepatitis p A: serologischer g Verlauf A Ki Kinetik tik Marker HBV Definition Bedeutung Hepatitis B: serologischer Verlauf Diagnostische g Marker Hepatitis-B pdirekter Virusnachweis Virus-DNA HBV-DNA HBsAg Oberflächenprotein akute/chronische Infektion, frühester Marker,, Infektiösität HBeAg ins Blut sezerniertes Virusprotein (teilweise identisch mit HBcAg) Infektionsmarker: hohe Infektiösität Anti-HBc Antikörper gegen HBcAg (IgG + IgM) Durchseuchungsmarker, lebenslang positiv nach HBVKontakt (akute/chronische, (akute/chronische abgelaufende Hep.-B) Anti-HBc-IgM Antikörper gegen HBcAg (IgM) hohe Titer beweisen akute Hep.-B-Infektion Anti-HBe Antikörper gegen HBeAg löst HBeAg ab; spricht für geringere/fehlende Infektiösität Anti-HBs Antikörper gegen HBsAg abgelaufende Hep.-B (in Verbindung mir Anti-HBc); Anti HBc); Immunität (einziger Antikörper nach Hepatitis-B-Impfung) - 9 - - 10 - Sceening eng Hepatitis D • Hepatitis Delta Virus • inkomplettes („nacktes“) Virus (Viroid), benötigt für Replikation Hülle des HBV (HBsAg) Hepatitis D Virus (HDV) korrespondierende Antikörper Hülle: HBsAg (Leih-Ag) anti-HBs Kern: HDV-Ag anti-HDV Kern: HDV-RNA Simultan-Infektion Si lt I f kti : HBV + HDV (selten, ( lt Heilung H il 90%) Super-Infektion : HBsAg-Trägers (häufig, fulminant/chronisch) - 11 - - 12 - Sceening breit B: Narbe - 13 - B: Impfung, unnötige Untersuchung - 14 - B: Narbe + C - 15 - - 16 - B: frisch? Oder isoliert B: Isoliert, dann geimpft - 17 - - 18 - B: Beide Antigene, PCR B: Narbe, starker Impftiter - 19 - - 20 - B: isoliert, Delta - 21 - B: Beide Antigene, PCR, Hepatitis Delta - 23 - - 22 - B: Rezidiv - 24 - Hepatitis C akut: Verlauf Hepatitis C chronisch: Verlauf Nachweisgrenze - 25 - - 26 - C: nur positiv C-Blot schematisch - 27 - - 28 - C: positiv + PCR C: schwach positiv - 29 - - 30 - 3 2 C: PCR qualitativ + quantitativ HIV: Western Blot 1 1 = Positive Kontrolle HIV: Blot 2 = Negative Kontrolle 3 = positiver Patient Nachweis von Antikörpern, die gegen verschiedene Epitope (Hülle Kern) des HIV (Hülle, HIV-Virus Virus gerichtet sind - 31 - - 32 -