Interpretation von serologischen Befunden
Werbung

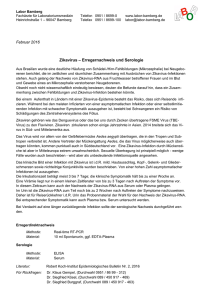
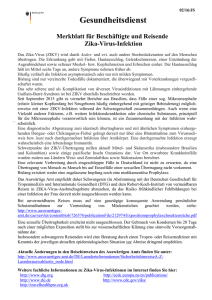
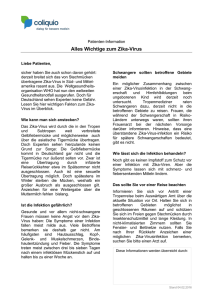
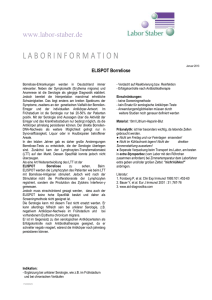
Interpretation von serologischen Befunden Cédric Hirzel Berner Infektiologie Symposium 2014 Hausärztliche serologische Fragen Borreliose HBV EBV Interpretation von serologischen Befunden • Epstein‐Barr‐Virus Serologie • HIV‐Serologie (Kinetik 4. Generationstest) • HBV‐Serologie Infektiöse Mononukleose EBV CMV HIV HHV‐6 Toxoplasmose Infektiöse Mononukleose Spezifische Serologie Monotest Epstein-Barr-Virus • Monotest (heterophile Antikörper): – Sensitivität abhängig von Symptomdauer 1: • 75% in erster Krankheitswoche • 95% in zweiter Krankheitswoche – Sensitivität abhängig vom Patientenalter 2: • 27% Kinder unter 2 Jahre • 76% Kinder über 2 Jahre – Hohe Spezifität 3: • 98‐100% 1) Am Fam Physician. 2004 Oct 1;70(7):1279‐1287 2) Blood. 1981 May;57(5):933‐8 3) Clin Diagn Lab Immunol. 2000 May;7(3):451‐6 Epstein-Barr-Virus • Virusspezifische Serologie: – Sensitivität 1: • 95‐100% • In der Regel früher positiv als heterophile AK • Kinder unter 2 Jahren geringere Sensitivität (63%) 2 – Spezifität 1: • 86‐100% 1)Clin Diagn Lab Immunol. 2000 May;7(3):451‐6 2)Blood. 1981 May;57(5):933‐8 Epstein-Barr-Virus Spezifische Serologie Monotest Epstein-Barr-Virus • • • • • • VCA: – Virus capsid antigen: virales Strukturprotein EA: – Early antigens: Proteine für Virusreplikation (Thymidinkinase, Polymerase) EBNA 1: – Epstein Barr nuclear antigen 1: Protein zur Aufrechterhaltung des EBV Episoms EBNA 2 und 3 – Epstein Barr nuclear antigen 2 und 3a‐c: Regulatorische Proteine (u.a. Lymphocytenimmortalisation) LMP 1 und 2: – Latent membrane protein 1 und 2: u.a. Schutz vor Apoptose MA: – Membrane antigen: u.a. gp350/gp220 viraler Rezeptor für Zellinvasion Epstein-Barr-Virus • • • • • • VCA: – Virus capsid antigen: virales Strukturprotein EA: – Early antigens: Proteine für Virusreplikation (Thymidinkinase, Polymerase) EBNA 1: – Epstein Barr nuclear antigen 1: Protein zur Aufrechterhaltung des EBV Episoms EBNA 2 und 3 – Epstein Barr nuclear antigen 2 und 3a‐c: Regulatorische Proteine (u.a. Lymphocytenimmortalisation) LMP 1 und 2: – Latent membrane protein 1 und 2: u.a. Schutz vor Apoptose MA: – Membrane antigen: u.a. gp350/gp220 viraler Rezeptor für Zellinvasion Epstein-Barr-Virus • EBV spezifische Antikörper: Schweiz Med Forum 2014; 14(11):226‐232 Epstein-Barr-Virus Expression von -BZLF1 -BRLF1 -VCA Epstein-Barr-Virus Expression von -LMP -EBNA Epstein-Barr-Virus Modifiziert nach Schweiz Med Forum 2014; 14(11):226‐232 Epstein-Barr-Virus VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + − − Frische Infektion / falsch pos IgM + + − Frische Infektion − + + Alte (latente) Infektion − − − Keine Infektion VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + + + ??? − + − ??? Modifiziert nach World J Virol 2012 February 12; 1(1): 31‐43 Epstein-Barr-Virus VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + − − Frische Infektion / falsch pos IgM + + − Frische Infektion − + + Alte (latente) Infektion − − − Keine Infektion VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + + + ??? − + − ??? Modifiziert nach World J Virol 2012 February 12; 1(1): 31‐43 Epstein-Barr-Virus • Alle Antikörper positiv: Epstein-Barr-Virus VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + − − Frische Infektion / falsch pos IgM + + − Frische Infektion − + + Alte (latente) Infektion − − − Keine Infektion VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + + + ??? − + − ??? Modifiziert nach World J Virol 2012 February 12; 1(1): 31‐43 Epstein-Barr-Virus • Isoliertes VCA-IgG: Epstein-Barr-Virus VCA-IgM VCA-IgG EBNA-1-IgG Interpretation + + + ??? − + − ??? Immunoblot hilft weiter 1: -frische Infektion: Anti-p54-IgM/G und Anti-p-138-IgM/G positiv -alte Infektion: Anti-p18-IgG (Anti-p18-IgG geht bei Immunsuppression nicht verloren) -Reaktivierung: Anti-p54-IgA und Anti-p138-IgA stark positiv 1) World J Virol 2012 February 12; 1(1): 31‐43 Epstein-Barr-Virus HIV‐Primoinfekt nicht vergessen HIV * * Späte primäre Infektion möglich wenn alle Ak positiv Modifiziert nach Schweiz Med Forum 2014; 14(11):226‐232 HIV 4. Generationstest • HIV 4. Generationstest: – Antikörper + p24 Antigen Nachweis N Engl J Med 2011;364:1943‐54 HIV 4. Generationstest Int J STD AIDS. 2014 Jul 16. pii: 0956462414542987. [Epub ahead of print] Hepatitis-B Serologie • Unklarheiten –Kein anti-HBs nach Impfung –Anti-HBc alone –HBeAg negativ / antiHBeAg negativ Fall Hepatitis-B Serologie • 32 jährige Patientin, IVDU • 3x Engerix geimpft • Anti-Hbs 4 Wochen nach 3. Impfung nicht messbar Wie weiter? Hepatitis-B Serologie A) Non‐Responder, nochmals Engerix B) Non‐Responder 3 Engerix, dann Titer C) HBs‐Ag bestimmen D) HBs‐Ag und anti‐HBc AK bestimmen E) HBe‐Ag, anti‐HBe AK und HBs‐Ag bestimmen F) Andere Lösung Hepatitis-B Serologie • Resultate Serologie: –HBsAg negativ –Anti-HBc Ak positiv –Anti-HBs Ak negativ, HBe negativ, anti-HBe AK negativ • „anti-HBc alone“ Hepatitis-B Serologie • Anti-HBc alone 1. HBV Infektion in der „window phase“ N Engl J Med 2004;350:1118‐29 Hepatitis-B Serologie • Anti‐HBc alone 1. HBV Infektion in der „window period“ 2. Okkulte HBV Infektion ‐Virale Genexpression ‐HBs Ag Mutante Journal of Hepatology 46 (2007) 160–170 Hepatitis-B Serologie • Anti‐HBc alone 1. 2. 3. 4. HBV Infektion in der „window period“ Okkulte HBV Infektion Falsch positives anti‐HBc 1 Falsch negatives (sehr tiefes) anti‐HBs 2 1) Arch Virol (2010) 155:149–158 2) Liver 2001: 21: 380–383 Hepatitis-B Serologie Arch Virol (2010) 155:149–158 Hepatitis-B Serologie Arch Virol (2010) 155:149–158 Hepatitis-B Serologie • 32 jährige Patientin, IVDU • 3x Engerix geimpft • Anti‐Hbs 4 Wochen nach 3. Impfung nicht messbar HBV DNA 1500 IU/ml HCV positiv Okkulte Hepatitis B • HBs Ag positiv, anti-HBc positiv, HBeAg negativ, antiHBeAg negativ N Engl J Med 2004;350:1118‐29 Hepatitis-B Serologie HBeAg G1896A Mutation Hepatitis-B Serologie Phase HBsAg Anti HBsAg HBeAg Anti HBeAg HBV DNA ALAT/ASAT Fibrose Progression Immuntolerant + - + - Keine/langsam Immunreaktiv HBeAg positiv + - + - schnell Inaktiver Carrier Status + - - + <2000IU langsam HBeAg negative CHB + - - +/- flukt flukt schnell HBsAG negative Phase - + - + 0 () keine Interpretation von serologischen Befunden • EBV‐Serologie – EBNA‐1 IgG als „Startpunkt“ zur Interpretation • Wenn positiv meist alte Infektion – Isoliertes VCA IgG • Immunoblot ermöglicht die Interpretation • HBV‐Serologie – Bei non‐Responder nach HBV Infektion suchen – Anti‐HBc alone • Cave „window phase“ und okkulte HBV Infektion