Problemkeime bei CF
Werbung

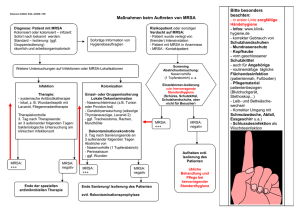
Problemkeime bei CF Burkholderia cenocepacia x35000 Dr. Tim O. Hirche Mukoviszidose-Erwachsenenambulanz Klinikum der J.W. Goethe Universität Frankfurt am Main CF Atemwegsinfektionen chronische Sinusitis chronische Infektion der unteren Atemwege CF Atemwegsinfektionen [%] Staphylococcus aureus Haemophilus influenzae Pseudomonas aeruginosa Burkholderia cepacia Complex Stenotrophomonas maltophilia Achromobacter xylosoxidans MRSA atypische Mykobakterien (Aspergillus fumigatus) Alter [J] aus: Cystic Fibrosis Foundation Patient Registry 2001 Opportunisten ! Korrelation Staph. aureus - Morbidität • Schlesinger et al. 1984. Effect of long term continuous anti-staphylococcal antibiotic treatment in young children with cystic fibrosis. Proc. 9th Int. CF Conf 4.14. • Chatfield et al. 1991. Neonatal screening for cystic fibrosis in Wales and the West Midlands: clinical assessment after five years of screening. Arch Dis Child 66:29-33 • Weaver et al 1994. Prognosis in cystic fibrosis treated with continuous flucloxacillin from the neonatal period. Arch Dis Child 70:84-89 • Stutman et al. 2002. Antibiotic prophylaxis in infants and young children with cystic fibrosis: A randomized controlled trial. J Pediatr 140: 299-305 Smyth et al. 2003. Prophylactic antibiotics for cystic fibrosis. Cochrane Database Syst Rev 2: CD001021 ! - signifikant geringerer Anteil Staph. aureus pos. in TX Gruppe - keine signifikanten Unterschiede LUFU, Ernährungstatus, KKH - signifikant höherer Anteil PA pos. in TX Gruppe MRSA und CF (CFF registry 7% MRSA pos. [center range 0-22%]) • Miall et al 2001. MRSA infection in cystic fibrosis. Arch Dis Child 84:160-162 • Thomas et al 1998. MRSA: Impact at national CF centers. J Hosp Infect 40: 203-209 • Boxerbaum et al 1988. Prevalence and significance of MRSA in CF patients. Pediatr Pulmonol 4:159-163 ! - MRSA häufig nur transient nachweisbar (35% <1Monat) - bei MRSA schlechtere base-line X-ray, LUFU, mehr iv-Antibiosen - keine dynamische Verschlechterung LUFU, Ernährungstatus, KKH • Schlichting et al 1993.Typing of Staph.aureus: resolution of clonal relationships. J Clin Microbiol 31:227-232 • Givney et al 1997. MRSA infection in a cystic fibrosis unit. J Hosp Infect 35:27-36 ! - Transmission MSSA und MRSA von nonCF-CF, CF-CF, CF-nonCF bewiesen - CF Patienten nicht empfänglicher als andere Patientengruppen - Standard Hygienevorschriften im Krankenhaus beachten Korrelation Pseudomonas - Morbidität • Henry et al. 1992. Mucoid Pseudomonas aeruginosa is a marker of poor survival in cystic fibrosis . Pediatr Pulmonol 12: 158-161 • Davis et al. 1995. Gender differences in cystic fibrosis Pseudomonas aeruginosa infection. J Clin Epidemiol 48: 1041-1049 • Ballmann et al. 1998. Long-term follow-up of changes in FEV1 and treatment intensity during Pseudomonas colonisation in patients with cystic fibrosis. Thorax 53:732-737 • Rosenfeld et al. 2001. Early pulmonary infection, inflammation, and clinical outcomes in infants with cystic fibrosis. Pediatr Pulmonol 32:356-366 • Nixon et al. 2001. Clinical outcome after early Pseudomonas aeruginosa infection in cystic fibrosis. J. Pediatr 138:699-704 • Gibson et al. 2002. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol 34:91-100 ! - Chronische PA Infektion verschlechtert LUFU, X-ray score, hospital days, 10-year survival .... - Nachweis mukoides Wachstum prognostisch deutlich ungünstiger Pseudomonas aeruginosa Transmission • CF–CF ausserhalb KKH: - CF Geschwister haben häufig (>50%) identischen PA - Transmission multiresistenter Stämme nach engem Kontakt Beispiel => Summer camp • CF–non CF ausserhalb KKH: Einzelfallberichte Infektionen mit virulenten Stämmen • CF–non CF innerhalb KKH: gesicherte Infektion immunsupprimierter Pat. • CF–CF über Ambulanz/KKH: Pro: Hoiby et al. 1999: Changing epidemiology of PA infection in Danish CF patients 1974-1995. Pediatr Pulmonol 28:159-66 200 isolates/60 pat: 2 strain clusters consisting of 26 and 11 Patients Implementierung von Hygienemassnahmen: weniger/späterer PA Erwerb Contra: Williams et al. 1997. Evaluation of antimicrobial sensitivity patterns as markers for PA cross infection in CF clinic. Br J Biomed Sci 54:181-5 469 isolate/69 Pat, kein identischer PA Speert et al. 2002. Epidemiology of PA in CF in British Columbia >500 isolates/153 Pat. PA pos, 133 unterschiedliche Stämme, 20 x Geschwister, 1x Freund ! - Transmission PA nach engem (körperlichen) Kontakt bewiesen - Transmission abhängig von der Virulenz des Keimes, Epidemien mit multiresistenten PA möglich Genus Burkholderia B.cenocepacia V II IX IV VII Burkholder 1950. Sour skin, a bacterial rot of onion bulbs. Phytopathology 40: 115-117 Burkholderia pseudomallei Holden et al. Proc Natl Acad Sci U S A. 2004 Coenye et al. 2001. Taxonomy and identification of the Burkholderia cepatia complex. J Clin Microbiol 39:3427-3436 Epidemiologie B. cepacia complex • LiPuma et al. 1998. Burkholderia cepacia epidemiology and pathogenesis. Curr Opin Pulm Med 4: 337-341 • LiPuma et al. 2001. Disproportionate distribution of Burkholderia cepacia complex species and transmissibility markers in CF. Am J Respir Crit Care Med 164: 92-96 • McMenamin et al. 2000. Misidentification of Burkholderia cepacia in US CF treatment centers. An analysis of 1051 sputum samples ! - Alle B. cepacia complex species wurden bei CF Patienten nachgewiesen - Prävalenz hohe regionale Variabilität (0-30%), overall USA/Europa <10% - Häufigkeit: B. cenocepacia (50%) > B. multivorans (35%) > Rest (15%) - Häufig falsch pos. (11%) / falsch neg. Befunde (36%) !? Korrelation B. cepacia - Morbidität • Isles et al. 1984. Pseudomonas cepatia infection in cystic fibrosis: an emerging problem. J Pediatr 104:206-210 • Talban et al. 1987. Colonisation of the respiratory tract with Pseudomonas cepacia in CF: Risk factors and outcomes. Chest 91: 527-532 • Sun et al. 1995. The emergence of a highly transmissible lineage of Burkholderia cepatia causing CF centre epidemics in North America and Britain. Nat Med 1:661-666 • Whiteford et al. 1995. Outcome of Burkholderia cepacia colonisation in children with CF following a hospital outbreak • Mahenthiralingam et al. 2001. Infection with Burkholderia cepacia complex genomovars in patients with CF. Clin Infect DIs 33: 1469-1475 ! - B. cepacia complex Infektion verschlechtert LUFU, hospital days, median survival… - „Cepacia Syndrom“: hohe Mortalität durch virulente/multiresistente Subspezies von B. cenocepacia und B. multivorans (z.B. ET12, Cbl Pili pos) Burkholderia cepacia Exposition • Häufiger Nachweis im Bereich landwirtschaftlicher Nutzflächen, seltener in Städten (Einsatz CF pathogener Spezies in der Landwirschaft zur Bodenverbesserung !) • Nachweis in Handcremes, Desinfektionslösungen, Inhalationslösung, Aqua dest. … • Humphreys et al. 1994. Airborne dissemination of Burkholderia cepacia from adult patients with CF. Thorax 49: 1147-49 Ensor et al. 1996. Is Burkholderia cepacia disseminated from CF patients during physiotherapy? J Hosp Infect 32: 9-15 => Vor Physio 16% Luftproben im Abstand von 1 Meter kontaminiert => Während Physio 44% Luftproben im Abstand von 1 Meter kontaminiert => Nachweis B. cepacia in Luftproben 15-45min nach Verlassen des Raums pos.! ! - Exposition gegenüber B. cepacia complex aus der Umwelt vermeidbar ? - Exposition bei Kontakt CF-CF (z.B. Station/Ambulanz) möglich. Vermeidbar ? Burkholderia cepacia Transmission • CF–CF ausserhalb KKH: - CF Geschwister nachgewiesen - Transmission nach sozialem Kontakt gesichert Beispiel => Summer camp, Autofahrt, Handschütteln, Essbesteck… • CF–non CF/nonCF-nonCF: CGD Patienten, Einzelfallberichte Infektion Vorgesunder ausserhalb KKH • CF–non CF innerhalb KKH: gesicherte Infektionen ventilierter Pat., Infektionen HCW! • CF–CF über Ambulanz/KKH: gesichert Nelson et al. 1991. Pseudomonas cepacia in inpatients with CF. Lancet 338:1525 Pegues et al. 1994. Possible nosocomial transmission of Pseudomonas cepacia in patients with CF. Arch Pediatr Adolesc Med 48: 805-812 ! - Transmission gesichert, nicht notwendigerweise an fortschrittenes Krankheitsstadium gebunden - Kontagiosität abhängig von der Virulenz des Keimes, Epidemien mit multiresistenten B. cenocepacia/B. multivorans nachgewiesen - Bei Nachweis/Verdacht Segregation notwendig Hygienemassnahmen bei CF • Saiman et al. 2003. Cystic Fibrosis Foundation Consensus Conference on infection control: participants: infection control recommendations for patients with cystic fibrosis: microbiology, important pathogens, and infection control practice to prevent patient-topatient transmission. Am J Infect Control 31:S1-S62 • Schewe et al. 2005. Instructions for infection control in outpatient care of patients with cystic fibrosis. Eur J Med Res 10: 345-351 => CF Ambulanz • Vonberg et al. 2004. Isolation measurements for CF patients [=Hygienemassnahmen für Patienten mit Cystischer Fibrose]. Pneumologie 58:309-315 => stationärer Aufenthalt Cave Hygieneempfehlungen bei CF • Ullrich et al. 2002. Parental fears of Pseudomonas infection and measures to prevent its aquisition. J Cyst Fibros 1:122-130 • Steinkamp & Ullrich 2003. Different opinions of physicians on the importance of measures to prevent acquisition of Pseudomonas aeruginosa from the environement. J Cyst Fibros 2: 199-205 ! - Empfehlungen zur sanitären Hygiene, Verhalten in Räumen, im Freien, Umgang Mitmenschen/Patienten, bei der Therapie etc… diffus, hohe Variabilität zwischen den Behandlern - Empfehlungen häufig ohne Evidence base - Empfehlungen können gravierenden Impact auf Verhalten/Lebensqualit der Patienten/Familien haben