Prof. Dr. G. Krastl: Wurzelresorptionen
Werbung

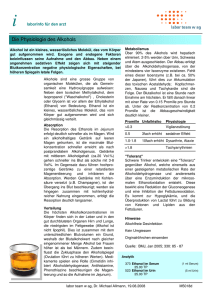
Wurzelresorptionen Physiologische Resorption ! Milchzahnresorption Wurzelresorptionen: Übersicht Gabriel Krastl Ursache: Druck durch Zahnkeim nicht alleiniger Faktor Obersztyn A Experimental investigation of factors causing resorption of deciduous teeth. J Dent Res 1963;42:660-674. Poliklinik für Zahnerhaltung und Parodontologie Direktor: Prof. Dr. G. Krastl Odontoklasten Osteoklasten • Gleicher Zelltyp wie Osteoklasten • Gleiche ultrastrukturelle Eigenschaften Furseth 1968; Yaeger and Kraucunas 1969; Sasaki et al. 1989; Matsuda 1992; Sahara et al. 1992 • Gleiche histochemische Eigenschaften Pierce A, Heithersay C, Lindskog S. Evidence for direct inhibition of dentinoclasts by a orticosteroid/antibiotic endodontic paste. Endod Dent Traumatol 1988 Freilich 1971; Hammarström et al. 1971; Matsuda 1992; Sahara et al. 1992; Sasaki and Ueno-Matsuda 1992 Kölliker, A. , "Die normale Resorption des Knochengewebes und ihre Bedeutung für die Entstehung der typischen Knochenformen" (Vogel, Leipzig, 1873) Quelle:http://www.unifr.ch/anatomy/elearningfree/allemand/stuetzgewebe/knochen/zellen/d-osteoklast.php Funktionsweise Osteoklasten • Auflösung der Calcium-Verbindungen durch Säure Osteoklasten Aktivierung • Sekretion von lysosomalen Enzymen für den Abbau der organischen Matrix 1 Osteozyt 3 Howship'sche Lakune 2 Knochenmatrix 4 mehrkerniger Osteoklast • Rezeptor-vermittelte Endozytose der MatrixFragmente RANKL (Receptor Activator of Nuclear factor Ligand) Regulation / RANKL Inaktivierung durch OPG (Osteoprotegerin) Versiegelungszone Faltensaum H+ monozytäre Osteoklastenvorläuferzellen mit RANK Rezeptoren Aktivierung durch RANKL Aggregation Fusion zu Osteoklasten Einflussfaktoren für Osteoklastenaktivität Knochen lebenslange Umbauprozesse (ca. 10% / Jahr) • Vorbeugung gegen Materialermüdung • funktionelle Anpassung an herrschende Belastung • Reparatur von Mikrotraumen • Rasche Mobilisierung von Calcium Quelle: Andreasen et al. 2007 . Textbook and Color Atlas of Traumatic Injuries of the Teeth Resorptionsschutz? Zahn 1. Netzwerk aus Epithelresten um die Zahnwurzel unter normalen Umständen kein Umbau / keine Resorption ORBAN B The epithelial network in the periodontal membrane. J Am Dent Assoc 1952;44:632-635. 2. Intrinsische Faktoren im Zement und Prädentin !OPG Levin L, Trope M. Root Resorption. In Selzer and Bender´s Dental Pulp, 2002;425-447. 3. Hoch kalzifiziertes intermediäres Zement als Barriere zwischen Dentinkanälchen und Parodont Trope M Root Resorption due to Dental Trauma. Endodontic Topics 2002;1:79-100. 4. Wurzelbedeckung: Präzement (Wurzeloberfläche) / Prädentin (Wurzelkanal) Trope M Root Resorption due to Dental Trauma. Endodontic Topics 2002;1:79-100. Kerr 1961, Raisz 1976; Hammarström und Lindskog 1985 Wurzelresorption Klassifikationenen Andreasen JO Luxation of permanent teeth due to trauma. A clinical and radiographic follow-up study of 189 injured teeth. Scand J Dent Res 1970;78:273-286. • • Interne Resorption Externe Resorption – Oberflächenresorption – Entzündliche Resorption – Ersatzresorption Tronstad L Root resorption--etiology, terminology and clinical manifestations. Endod Dent Traumatol 1988;4:241-252. • Transiente entzündliche Resorptionen • Progressive entzündliche Resorptionen – Interne Resorption – Externe Resorption • Progressive externe entzündliche Resorption • • Zervikale Resorption Ankylose /Ersatzresorption • • Interne Resorption Externe Resorption – Externe Oberflächenresorption – Externe entzündliche Resorption – Ankylose – Externe Ersatzresorption • • Cervikal • Apikal Transiente apikale Resorptionen Trope M (2002). Root Resorption due to Dental Trauma. Endodontic Topics 1(1):79-100. • • • Protective layer damage + pressure (orthodontic movement, impacted teeth, tumor) Protective layer damage + pulp space infection Protective layer damage + sulcular infection Fuss Z, Tsesis I, Lin S (2003). Root resorption--diagnosis, classification and treatment choices based on stim. factors. Dent Traumatol 19(4):175-182. Benenati FW Root resorption: types and treatment. Gen Dent 1997;45:42-45. • Interne Resorption – Entzündlich – Supraossäre Perforation – Intraossäre Perforation • Externe Resorption – Transiente Resorptionen • Oberflächenresorption • Druckresorption – Pathologisch • Ersatzresorption • • Entzündliche Resorption Extrakanaläre invasive Resorption • Iatrogene resorption Wurzelresorptionen - Klassifikation Ne RF, Witherspoon DE, Gutmann JL. Tooth resorption. Quintessence Int 1999;30:9-25. • • • • • Wurzelresorption durch Pulpainfektion Wurzelresorption durch parodontale Infektion Wurzelresorption durch KFO Kräfte Wurzelresorption durch Druck impaktierter Zähne oder Tumoren Ankylotische Wurzelresorption Pizzo G, Licata ME, Guiglia R, Giuliana G. Root resorption and orthodontic treatment. Review of the literature. Minerva Stomatol 2007;56:31-44. • Orthodontisch induzierte entzündliche Wurzelresorption – Oberflächenresorption – – Tiefe Resorption Zirkumferente apikale Resorption 1. TRAUMA BEDINGT • Unfall • Paro-Therapie/Chirurgie • KFO (Druck) • Impaktierter Zahn (Druck) • Zyste/Tumor (Druck) 2. INFEKTIONSBEDINGT • Infektion im Wurzelkanals 3. HYPERPLASTISCH-INVASIV BEDINGT • invasives Gewebe Resorptionsart Ursache Externe transiente Resorption Räumlich begrenzter mechanischer Wurzelzementschaden Wurzelresorptionen - Klassifikation Externe transiente Resorption 1. TRAUMA BEDINGT • Unfall • Paro-Therapie/Chirurgie • KFO (Druck) • Impaktierter Zahn (Druck) • Zyste/Tumor (Druck) Oberflächenresorptionen nach Zahntrauma • Räumlich begrenzte, mit Zement ausgekleidete Wurzelresorptionen Resorptionsart Ursache Externe transiente Resorption Räumlich begrenzter mechanischer Wurzelzementschaden Externe Ersatzresorption (Osseous replacement) Massiver Wurzelzementschaden (> 20% der Wurzel) 2. INFEKTIONSBEDINGT • Infektion im Wurzelkanals • Keine klinische Bedeutung • Bleiben im Rx-Bild häufig unentdeckt 3. HYPERPLASTISCH-INVASIV BEDINGT • invasives Gewebe Externe Ersatzresorptionen Med. Avulsion 21 + 2 Wochen + 4 Wochen Ersatzresorptionen (osseous replacement) WF + 8 Monate • Voraussetzung: ausgedehnte Nekrosen des parodontalen Ligaments • Wurzel wird innerhalb von Jahren resorbiert und durch Knochen ersetzt • Folge: Ankylose, evtl. Infraposition des Zahnes bei Pat. im Wachstum + 14 Monate + 3 Jahre + 4 Jahre + 6 Jahre Progression der Ersatzresorptionen Resorptionsindex Andersson, L., I. Bodin, et al. (1989). "Progression of root resorption following replantation of human teeth after extended extraoral storage." Endod.Dent.Traumatol. 5(1): 38-47. 12 8 4 0 Zustand 6 Jahre nach Replantation 21 Patient damals 12 Jahre alt, Trockenlagerung 21: 1h Alter 8-16 Alter 19-37 1 3 6 12 24 Monate 48 96 150 Wurzelresorptionen - Klassifikation 1. TRAUMA BEDINGT • Unfall • Paro-Therapie/Chirurgie • KFO (Druck) • Impaktierter Zahn (Druck) • Zyste/Tumor (Druck) 2. INFEKTIONSBEDINGT • Infektion im Wurzelkanals 3. HYPERPLASTISCH-INVASIV BEDINGT • invasives Gewebe Resorptionsart Ursache Externe transiente Resorption Räumlich begrenzter mechanischer Wurzelzementschaden Externe Ersatzresorption (Osseous replacement) Massiver Wurzelzementschaden (> 20% der Wurzel) Externe infektionsbedingte Resorption Wurzelkanalinfektion + Wurzelzementschaden Schädigung Parodont Schädigung Endodont • Direkte Traumafolge • prolongierte extraorale Aufbewahrung des Zahns • Zahnauslenkung, Zerrung, Ruptur der Pulpa • Bakterielle Invasion Externe Wurzelresorptionen Transiente Resorptionen Ersatzresorptionen Infektionsbedingte Resorptionen Wurzelkanalinfektion Infizierte Pulpanekrose Apikale Parodontitis Infektionsbedingte Wurzelresorptionen Externe infektionsbedingte Resorption Befunde bei infektionsbedingten Resorptionen • Voraussetzung: Areale mit nektrotischem Wurzelzement + Infektion des Wurzelkanals • Schnell fortschreitende Dentinresorptionen führen zur Zerstörung der Wurzel innerhalb von Monaten Klinisch • fehlende Reaktion auf den Sensibilitätstest, ansonsten anfangs meist keine Hinweise. • in späteren Stadien erhöhter Lockerungsgrad mit dumpfem Perkussionsschall, Perkussionsempfindlichkeit sowie Fistelbildung möglich Befunde bei infektionsbedingten Resorptionen Therapie infektionsbedingter Resorptionen • Ziel:&Elimina+on&der&intrakanalären&Infek+on&(Langzeiteinlagen?) • Extrak+on&bei&sehr&stark&ausgeprägten&Resorp+onen Radiologisch • transluzente Zonen unterschiedlicher Größe entlang einer unregelmäßigen Außenkontur, sowohl in der Wurzel als auch im benachbarten Knochen („schüsselförmige“ Resorptionslakunen). Wie wirkt Calciumhydroxid bei infektionsbedingten Resorptionen? Andreasen JO, Farik B, Munksgaard EC (2002). Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. DentTraumatol 18(3):134-137. „Versprödung“ des Dentins bei Langzeiteinlagen aber keine signifikante Veränderung der Frakturresistenz nach Ca(OH)2 et al. Einlagen bis zuAndreasen 30 Tagen Tronstad L, Andreasen JO, Hasselgren G, Kristerson L, Riis I (1981). pH changes in dental tissues after root canal filling with calcium hydroxide. Journal of endodontics 7(1):17-21. ➡ antibakterieller Effekt ➡ Neutralisierung der Säuren ➡ Inaktivierung der sauren ➡ OHOH- Hydrolasen (Cathepsin) Aktivierung der alkalischen Phosphatase ➡ früher als Langzeiteinlage (für mehrere Monate) empfohlen OHOHOHOH- Fig. 1. Reduction immature sheep te hydroxide. The lin FS ¼ 7.2 þ e(2.16#0. fracture strength, stant, and d, day The coefficient of e was obtained by assuming a ¢rst order kinetic and of dentin by calcium hydroxide according to the equation, and this value was estimated as the value giving a coe⁄cient of estimation, R2 closest to 1; in this case 0.95. According to the equation, the fracture strength for teeth containing properties of dentin. It has recen that sodium hypochlorite irrigat reducedthe modulus ofelasticitya of dentin (20), and the ¢nding was the assumption thatEinlagen the strength time beschränken This would leave the dentin stru Dauer der Ca(OH) aufwith 1 Monat ➡ Kompromiss:with 2 reached a certain plateau. The plateau is 7.2 MPa organic support, which may in£ue Resorptionsrisiko bei Dislokationsverletzungen? Andreasen&FM,&Pedersen&BV&(1985).&Prognosis&of&luxated&permanent&teethMMthe&development&of&pulp&necrosis.&Endod%Dent%Traumatol&1(6):207M220. 90 75 60 45 30 15 0 Konkussion (n=178) 17.12.07 Pulpanekrose Wurzelresorptionen - Klassifikation 1. TRAUMA BEDINGT • Unfall • Paro-Therapie/Chirurgie • KFO (Druck) • Impaktierter Zahn (Druck) • Zyste/Tumor (Druck) 2. INFEKTIONSBEDINGT • Infektion im Wurzelkanals 3. HYPERPLASTISCH-INVASIV BEDINGT • invasives Gewebe Resorptionsart Ursache Externe transiente Resorption Räumlich begrenzter mechanischer Wurzelzementschaden Externe Ersatzresorption (Osseous replacement) Massiver Wurzelzementschaden (> 20% der Wurzel) Externe infektionsbedingte Resorption Wurzelkanalinfektion + Wurzelzementschaden Interne infektionsbedingte Resorption Wurzelkanalinfektion mit vitalem Gewebe im Bereich der Resorption Lockerung (n=223) Transiente Resorptionen Extrusion (n=53) Lat. Dislokation (n=122) Infektionsbedingte Resorptionen Intrusion (n=61) Ersatzresorptionen Interne Resorption ➡ ➡ Prävalenz: 0,01% bis 1% der Patienten meistens nur 1 Zahn pro Patient betroffen MARKUS HAAPASALO & UNNI ENDAL Internal inflammatory root resorption: the unknown resorption of the tooth. Endodontic Topics 2006 Qu resorption in its most classical form spreads symmeothers to be involved in the initiation and pathogenesis involves release of calcium from bones (8). Pathological trically in all directions into the dentin surrounding the of internal inflammatory root resorption. overproduction of PTH, hyperparathyroidism, will pulp. The initiation of internal root A resorption l result in imbalance in the physiological bone resorption chen Interne Resorptionen le throughout the full circle of dentin at certainRedepths Interne Resorption: Ursachen? Interne Resorption – apposition cycle, and can cause radiolucent hyperparcht e athyroidism lesions in the jaws [see, e.g. (9–12)]. PTH v Kockapan C (2006). Das interne Granulom - Eine Übersicht. Endodontie 15(4):345-365. in the coronal-apical direction can perhaps be explainedor Histological features of internal be and PTH-related protein (PTHrP) induce spontaneous either by a slowly advancing pulpitis (inflammation) or halte ➡ chronischePulpitiden inflammatory resorption osteoclast formation and are required for tooth nt n Voraussetzungen by mechanical trauma. However, the fact remains that eruption (13, 14). e ss e n z ➡ Trauma Schaden des Prädentins ➡ Resorption of primary teeth is another relatively wellReports of the histological and microanatomical inflammatory restaurative Massnahmenroot resorption is rare and the ➡ internal characterized example of physiological resorption (15, Zerstörung der16). Odontoblastenschicht features of internal ➡ tooth resorption are based of information Silikatfüllungen, Silbernitraton it is scarce. Thus, the key ➡ amount Pressure fromon the permanent teeth is the driving force for resorption direktePulpaüberkappung Entzündung ➡ Pulpale examination of extracted teeth with ‘naturally occur- of the roots of primary teeth. in the initiation of internal inflammatory root ➡ events complex network of events on a cellular level Pulpotomie remain largely unknown. ➡ resorption ring’ internal resorptions on Aincluding experimentally Pulpagewebe am Ort der ➡ vitalesand several activating and inhibiting cytokines ➡ Kroneninfrakturen induced resorptions in Resorption animal modelsand(68, 73). is required to direct the Irrespective of the possible initiating factor (trauma, other72, compounds kieferorthopädische Behandlung ➡ inflammation resorption to the primary tooth and the bone while Allen & Gutmann (72) describedkoronal highly der vascularized or some other reason), there is a general Resorption ➡ Gewebe protecting the permanent developing tooth from ➡ erblicheFaktoren pulpal connective tissue infiltrated agreement that the progress of internal root resorption nekrotischby lymphocytes resorption. It is and important to note that there is no ➡ Schwangerschaft infectious (microbiological) component in the various plasma cells as well as ‘resorptive bays.’ Wedenberg & is dependent on two things: the pulp tissue at the ➡ Bakterieller Stimulus ➡ Herpeszoster types of physiological resorption. Zetterqvist (73) examined 13 primarysolange and permanent area must be vital, and the pulp coronal to Vitamin-A-Mangel ➡ resorption Durchblutung ➡ Progredienz of internal resorption. The resorption must be partially or completely necrotic, Hyperparathyreoidismus. ➡ the Kockapan C (2006). teeth extracted becausegesichert resorbing hard tissues the resorption allowing bacterial infection and microbial antigensdestoZahns authors reported that the progress ofCells der kieferorthopädischen Behandlung angefertigte OPG Abb. 11 Röntgenaufnahme n. 11 mit zwei separaten internen ResorpBildung von Granulationsgewebe und was faster in primary teeth, but that there were noare other enter the root canal (Fig. 3).tionen. Microbial stimulus is Osteoclasts multinuclear cells responsible for Differenzierung von Zellen zu vielkernigen resorption of bone, while odontoclasts are corresponddifferences between the two groups of teeth. The pulp necessary for the continuation of internal inflammatory MARKUS HAAPASALO & UNNI ENDAL Internal inflammatory root ing cells resorbing dental hard tissues (17–19). The Riesenzellen („Dentinoklasten“) Interne Resorption resorption showed hyperemia resorption: the unknown resorption of the tooth. Endodontic Topics 2006 tissue next to the multinuclear cellsand are formed by fusion of mononuclear (Fig. 1). Microscopic varying degrees of inflammation andcells infiltration of studies of odontoclasts using n der Wurzel gekommen ist. Hier Das circa 18 Monate alte OPG zeigte keine Auffälthree-dimensional reconstruction have shown that eister et al.128 zeigen, dass die An- ligkeiten (Abb. 10). Der Patient war beschwerdefrei,lymphocytes, macrophages, and neutrophilic leukoneral Trioxide Aggregate (MTA) als hatte aber die rötliche Verfärbung des Zahns be-cytes. Bacteria were detected histologically only in the d anzusehen ist. Es ist zu überlegen, merkt. Daraufhin suchte er seinen Hauszahnarzt auf,teeth undergoing rapidly progressing resorption. The ung von MTA zum Verschluss von der eine Röntgenaufnahme des Zahns anfertigte undbacteria were located either in the dentinal tubules or in internen Resorptionen sinnvoll und eine interne Resorption des Zahns 11 feststellte (Abb.the necrotic part of the coronal root canal. Interestbar ist. In der Literatur liegen bisher 11). ingly, the authors reported osteoid or cementum-like chte über dieses Thema vor129,130. tissue in some areas of the pulpal wall as well as small erwähnen, dass regelmäßige klinicalcifications in the pulp tissue. Odontoblast cells were ogische Kontrollen nach dentalen ! Befund erlich sind, um interne Resorptionen Die klinische Untersuchung ergab ein kariesfreies Ge-not detected in the resorption area in any of the teeth, biss. Der Zahn 11 war rötlich verfärbt (Abb. 12a undand predentin was also absent in most areas. Neutroitig zu entdecken75. b). Die Sensibilitätstestung mit CO2-Schnee verliefphils and macrophages were seen attached to the an den Zähnen 12, 11, 21 und 22 positiv. Der Per-mineralized dentin surface, and numerous odontoclasFig. 1. A histological kussionstest war an den Frontzähnen unauffällig. Beitic cells (see Fig. 1) were present in resorption lacunaespecimen showing an odontoclast llung cell with a high number of nuclei next to a resorbed dentin Bildung von Granulationsgewebe und der klinischen keine Auffäl-(73). Scanning electron Fig. 3. (a) A schematic drawingUntersuchung showing thekonnten pathogenesis surface. Hematoxylin eosin staining. Courtesy of Dr. P.-L. microscopy (SEM) of the Lukinmaa.zu vielkernigen zt stellte bei einem 15-jährigen Pa- ligkeiten im Bereich der Wurzeloberfläche festgeDifferenzierung von Zellen i several mon undergo fu with multin clasts can although du several nuc osteoclasts h (22) showe resorption, was 5.3, an mononucle ture have sh cementum Close simila ted. A study acid phosph teinase-9 i physiologic teeth found expression (18). Based and odonto difference b action in the cellular reso Regulat odontoc Osteoclasts of PTH, th PTH is ind bone formin ‘Receptor A (RANKL), osteoclast p osteoclasts (OPG) is a the tumor and has a v regulation o of osteoclas biting the RANK recep (24–26). Fu ontal ligam gical root r OPG expre MARKUS HAAPASALO & UNNI ENDAL Internal inflammatory root Haapasalo & Endal resorption: the unknown resorption of the tooth. Endodontic Topics 2006 Fig. 4. A scanning electron micrograph of the dentin surface treated with hypochlorite (to remove organic debris) after resorption. The micrograph shows resorbed dentin with numerous shallow resorption lacunae, which indicate the site of odontoclast activity. The small openings are dentinal tubules. Interne Resorption DVT besser geeignet variation of the common type of A histological als MF zur Detektion internal root resorption has also been suggested in kleiner interner the literature. Ne et al. (74) described root canal Resorptionen sowie replacement resorption (metaplastic resorption) which zur Beurteilung einer of dentin around the root canal and involved resorption möglichen Perforation subsequent deposition of osteoid or cementoid hard tissue. The authors reported that root canal replacement resorption can occur where there is chronic Bhuva B, Barnes JJ, Patel S (2011). The use of limited inflammation next to an area where damage to cone beam computed tomography in the diagnosis and management of a case of perforating internal root odontoblast cells and predentin has exposed the resorption. International endodontic journal 44(8): 777-786 mineralized dentin. However, it may be difficult to detect the difference between revascularization and subsequent formation of osteoid tissue from root canal replacement resorption. Kamburoglu K, Kursun S, Yuksel S, Oztas B (2011). Observer ability to detect ex vivo simulated internal or external cervical root resorption. Journal of endodontics 37(2):168-175. Interne Resorption (76) reported internal root resorption in eight out of KlinischeinZeichen 28 teeth (28%) where pulpotomy the coronal pulp • Zahn in der(covered Regel asymptomatisch, and capping with calcium hydroxide by zinc oxide eugenol) had beenPulpitissymptome performed. The teeth were möglich extracted 49–320 days after the endodontic procedures • bei ausgeprägter Resorption im and subjected to a histological study. Ahlberg et al. (77) spot“ koronalen Bereich: „pink reported a long-term evaluation of autotransplanted maxillary canines with an average follow-up time of Zeichen 6 years. Of the 33 teeth Radiologische included in the study, 17 (55%) • meistens runde oder ovale, developed internal resorption. Interestingly, no internal resorption was detected during the first year after symmetrische Erweiterterung des autotransplantation, and Wurzelkanals the majority of resorptions appeared 3 years or more after the procedure. The teeth were endodontically treated after the resorption was diagnosed. Many cases that have been referred to endodontic Bildung von Granulationsgewebe und specialists or university clinics as internal root resorpvon Zellen zu vielkernigen tions have turned out to Differenzierung be external cervical resorpRiesenzellen („Dentinoklasten“) tions. It should also be kept in mind that the diagnosis of internal root resorption is mainly based on radiographs, which means that a considerable amount of WKB root canal wall dentin must be resorbed to be reliably starke Blutung zu erwarten detected in the radiograph.➡ In oftmals cases where the root canal infection proceeds rapidly the root canal, komplette Entfernung des Gewebes ➡ through resulting in necrosis of the whole pulp, the resorption ➡ vorzugsweise NaOCl > 1% (if present) stops at an early stage and would remain Ultraschallaktivierte Spülung ➡radiographically. undetected both clinically and ➡andCa(OH) Based on the limited studies clinical experience 2 EInlageof the authors, we suggest a prevalence of between 0.01% Guttapercha, bei perforierten ➡ WF mit warmer and 1% (patients affected) for internal inflammatory Resorptionen MTA root resorption. Although this estimate is quite rough and may be wrong, it is unlikely that it will be replaced in the near future with a more correct figure that would be based on an epidemiological study. Typically, only one tooth per patient is affected by internal root resorption. However, occasionally two adjacent teeth have internal root resorption, with trauma being the Therapie interner Resorptionen Wurzelresorptionen - Klassifikation 1. TRAUMA BEDINGT • Unfall • Paro-Therapie/Chirurgie • KFO (Druck) • Impaktierter Zahn (Druck) • Zyste/Tumor (Druck) 2. INFEKTIONSBEDINGT • Infektion im Wurzelkanals 3. HYPERPLASTISCH-INVASIV BEDINGT • invasives Gewebe + 6 Monate Literatur Krastl / Weiger 1 Externe Wurzelresorptionen nach Dislokationsverletzungen Gabriel Krastl, Roland Weiger Externe Wurzelresorptionen nach Dislokationsverletzungen Transiente Resorption, infektionsbedingte Resorption, Ersatzresorption, invasive zervikale Resorption Gabriel Krastl Roland Weiger Wurzelresorptionen als mögliche Folge von Dislokationsverletzungen können die Prognose der betroffenen Zähne deutlich beeinträchtigen. Ihre Wahrscheinlichkeit nimmt mit dem Schweregrad der traumatisch bedingten parodontalen Schädigung zu. Während kleinere Areale des Wurzelzements regenerieren können (transiente Resorptionen), ist bei massiver Schädigung keine parodontale Heilung mehr zu erwarten. Ersatzresorptionen führen zum Ersatz des Dentins durch Knochen. Hat sich gleichzeitig eine Infektion des Endodonts etabliert, ist mit infektionsbedingten Resorptionen zu rechnen. Diese können in kurzer Zeit zur Auflösung der gesamten Wurzel führen. Vor diesem Hintergrund kommt einem adäquaten endodontischen Management eine große Bedeutung zu. Biologische Grundlagen Wurzelresorptionen sind die Folge odontoklastischer Zellaktivität1. Die Odontoklasten (auch Dentinoklasten genannt) gehören als mehrkernige phagozytische Zellen dem gleichen Zelltyp an wie Osteoklasten. Allerdings sind sie etwas kleiner und weisen weniger Zellkerne auf2. Die resorptive Auflösung von Hartgeweben erfolgt nach einem typischen Muster3: 1. Adhäsion der Zelle an der Hartsubstanz. 2. Aufbau einer dichten Versiegelungszone über dem Hartgewebe. 3. Bildung eines Bürstensaums innerhalb der Versiegelungszone. 4. Sezernierung von HCl und proteolytischen Enzymen. 5. Auflösung der anorganischen Kalziumverbindungen und enzymatische Spaltung der organischen Substanz mit Entstehung von Howship-Lakunen. 6. Abtransport organischer und anorganischer Abbauprodukte durch Transzytose. Die Regulation der Osteoklastenaktivität ist ein komplexer Vorgang und wird durch eine Vielzahl von Hormonen, Zytokinen und Wachstumsfaktoren beeinflusst3. Während die Resorption von Milchzahnwurzeln als physiologischer Prozess zu verstehen ist, liegt jeder Resorption an bleibenden Zähnen eine Pathologie zugrunde. Aus welchem Grund Zähne der zweiten Dentition nicht in die Umbauprozesse des Knochens mit eingebunden werden, ist bis heute nicht vollständig geklärt. Zur Erklärung der resorptionsinhibierenden Mechanismen an der Wurzeloberfläche existieren verschiedene Theorien. Der entscheidende Beitrag zur Verhinderung von Wurzelresorptionen wird dabei dem Wurzelzement zugesprochen. Zum einen bildet er eine mechanische Barriere, welche verhindert, dass mikrobielle Toxine bei Vorhandensein einer intrakanalären Infektion via Dentintubuli in das Parodont austreten. Zum anderen wird die Osteoklastenadhäsion an der äußeren Zementschicht aufgrund der fehlenden Mineralisation unterbunden4. Endodontie 2012;21(1):00–00 Kontaktadresse: Dr. Gabriel Krastl E-Mail: [email protected] Manuskript Eingang: 19.10.2011 Annahme: 03.11.2011 Resorptionsart Ursache Externe transiente Resorption Räumlich begrenzter mechanischer Wurzelzementschaden Externe Ersatzresorption (Osseous replacement) Massiver Wurzelzementschaden (> 20% der Wurzel) Externe infektionsbedingte Resorption Wurzelkanalinfektion + Wurzelzementschaden Interne infektionsbedingte Resorption Wurzelkanalinfektion mit vitalem Gewebe im Bereich der Resorption Externe invasive zervikale Resorption Trauma? KFO? Bleaching? Zementschaden + Sulkuläre Inf.?