Schnittstelle_Gynaekologie_Plastische_Chirurgie
Werbung

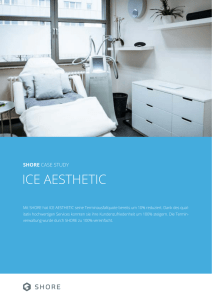
Schnittstelle Gynäkologie Plastische Chirurgie Maria Deutinger, D. Hoch, H. Klepetko, R.Bartsch, N. Gösseringer, M. Kaltseis Abt. für Plastische und Wiederherstellungschirurgie Krankenanstalt Rudolfstiftung Prim. Prof. Dr. Maria Deutinger Themen • • • • • • Augmentation Mammahyperplasie Bet Lipofilling Rekonstruktion Labienkorrektur Eingriffe an der Brust – was ist zu beachten? • Wunsch der Patientin • Ästhetisches Ergebnis • Therapeutisches Konzept Kapselfibrose - Literatur • Capsular Contractures: A Systematic Review • • Araco A., Caruso R., Araco F., Overton J., Gravante G., PRS 2009 Dec;124(6): 1808-19 • Kapselfibrose: 1, : 1,3% – 30% ► 92 % in den ersten 12 Monaten • 3% – 30% ► 92 % in den ersten 12 Monaten Einteilung nach BAKER : Grad I: Stadium ohne sichtbare oder tastbare Kapselfibrose. Grad II: minimale Kapselfibrose kaum feststellbar. diskrete Verhärtung der Brustimplantate zu ertasten. Grad III: Leichte Kapselfibrose - Die Patienten fühlen eine gewisse Spannung oder Festigkeit. Grad IV : Sofort sichtbare starke Kapselfibrose teils mit Schmerzen. Kapselfibrose - Literatur • Abhängig von: • Art der Operation: Rekonstruktion / Augmentation • ► höheres Risiko bei Rekonstruktion (10,4%) • • • ► höheres Risiko bei Radiatio Kapselfibrose ohne Radiatio: Kapselfibrose nach Radiatio: • 0% – 40% 32% – 70% Kapselfibrose - Literatur • Art des Implantates: texturiert – glatt • ► Risiko geringer bei texturierter Prothese • Positionierung des Implantates: subglandulär – submuskulär • • • • • ► Risiko höher wenn subglandulär Studie v. Gutowski: 500 Patientinnen > 8x höher bei subgland.Mammaaugm. ► Risiko ↓↓ je mehr Gewebe über dem Implantat, je weniger Kontakt zum Drüsengewebe Kapselfibrose - Literatur • Vorbeugende Maßnahmen: • ► Kohäsivgel gefüllte Implantate • ► Manipulation intraoperativ vermeiden • ► Perioperativ AB i.v. Mammahypertrophie – MRT estimated probability 0,8 0,7 0,6 v 0,5 Möglichkeit des Auftretens eines WS-Schadens bzgl. der Brustgröße 0,4 32 % 0,3 1750 g 0,2 Beidseitiges Brustgewicht (g) 0,1 0 0 1000 2000 3000 4000 Mammahypertrophie Kriterien für Kostenübernahme: • BMI 26 • Resektionsgewicht 500g/Seite •Körbchengröße > D Mammahypertrophie Rückenbeschwerden 100 80 60 VAS - SKALA 40 20 0 Über 500g Präoperativ Unter 500g Postoperativ Mammahypertrophie Stillen postoperativ • Breast feeding after aesthetic mammary operations • and cardiac operations through horizontal • submammary skinincision • Surg Gynecol Obstet 1993 Mar; 176(3): 267-70 • Deutinger M, Deutinger J. Mamma CA - Mammahypertrophie ► BET - Reduktion bds ► Technik je nach Tumorsitz Eingriffe an der Brust - Mamma CA Onkologische Sicherheit Rekonstruktion Kosmesis Zeitpunkt - Möglichkeiten Mamma CA 70 – 80 % BET 20 – 30 % Mastektomie Sofortrekonstruktion MRM (Modifiziert radikale Mastektomie) Spätrekonstruktion SSM (Skin Sparing Mastektomie) Areolasparing Mastektomie Zeitpunkt - Möglichkeiten Sofortrekonstruktion • Erhalt Submammarfalte, Brusthaut • Möglichkeit der primär ästhetischen Schnittführung • Weniger Operationen erforderlich / Weniger Kosten Spätrekonstruktion • Wunsch der Patientin • Medizinischer Grund Zeitpunkt – Entscheidung der Patientin Sofortrekonstruktion • Wahrung des Körperbildes • Kein weiterer Eingriff Spätrekonstruktion • Entscheidung der Patientin • Keine Aufklärung bezügl. • Sofortrekonstruktion Patientinnen - Zufriedenheit 0 = nicht zufrieden 1 = zufrieden 120 Ø 93% 100 80 MRM+Reko SSM+Sofortreko 60 40 20 0 0 1 Sofortrekonstruktion (SSM) – onkologische Sicherheit Authors Year No.patients L.R. (%) Follow UP (months) Slavin et al 1998 51 2.0 45 Newman et al 1998 372 6.2 26 Simmons et al 1999 77 3.9 60 Toth et al 1999 50 0 51.5 Kroll et al 1999 114 7.0 72 Rivadeira et al 2000 71 5.1 49 Foster et al 2002 25 4.0 49 Medina-Franco et al 2002 176 4.5 73 Carlson et al 2003 539 5.5 65 Spiegel et al 2003 177 5.6 118 Gerber et al 2003 112 5.4 59 Downes et al 2005 38 2.6 53 Sofortrekonstruktion (SSM) – Rezidivrate Jahr Anzahl Ø Alter Rezidive (%) F/U (months) 2004 3 47,3 0,0 46 2005 11 43,7 0,0 38 2006 10 45,9 0,0 25 2007 11 41,6 0,0 12 TOTAL 35 44,9 0,0 25 Nippel – sparing Mastektomie? • • • • Nipple – Sparing Mastectomy and Immediate Tissue Expander/Implant Breast Reconstruction Constancer m Chen et al PRS 2009 Dec;124(6): 1772-80 • 115x Mastektomie bei 66 Patientinnen + Sofortreko mit Expander/Implantat • >75x prophylaktisch • >49x therapeutisch bei Mamma CA • • > 111 Nippel – sparing > 4 Areola – sparing DIEP + Perforator CT • Präoperative Darstellung der Perforator-Gefäße am Abdomen mittels CT Angiographie • beim DIEP (Deep-Inferior-Epigastric-Perforator-Flap) CT - Angiographie • Verbesserung der Reliabilität des Lappens • bei verkürzter Op-Dauer •▼ • Routine im klinischen Alltag Eingriffe an der Brust – Lipofilling Korrekturen Vergrößerung Brust Asymmetrie Rekonstruktion Lipofilling Die Korrektur von Konturdefekten der weiblichen Brust reicht bis in 19. Jh. 1895 Czerny Plastischer Ersatz der Brustdrüse durch ein Lipom Zentralbl. Chir. 27:72, 1986 Sydney R Coleman Lipofilling Gesicht 2007 Coleman Brustvergrößerung mit Eigenfett 2008 Zocchi und Delay Seit 2007 Überreiter: prospektive kontrollierte Studie Lipofilling • • • 25 Patientinnen (Alter ø 49 Jahre; min. 18, max. 70 Jahre) Durchschnittlich 2 Eingriffe pro Patientin ( 1 – 4 Eingriffe) Nachuntersuchungszeitraum: Januar 2007 bis 2009 • • • • • • Indikationen: 15 Konturdefekte 3 Kapselfibrosen 3 Narbenadhaesionen 2 Radioderme 2 Mamma CA (Rekonstruktion) Lipofilling - Absaugung Infiltration mit Ringer-Lsg+Xylo+Epi Absaugung mittels 10 ml Spritze Lipofilling - Infiltration eventuell Lösung von Narben stumpfe Infiltrationskanülen ! nur Stichkanal auffüllen Kontaktfläche ! Lipofilling - BODYJET Absaugung + Aufarbeitung + Infiltration Lipofilling - Dokumentation □ Entnahmestelle und Menge Gesamt ml Abdomen Hüfte: rechts links Trochanter: rechts links Knie: rechts links □ Infiltrierte Gesamtmenge Lokalisation re li kontrollierte Studienbedingungen ! Rekonstruktion mit Lipofilling St.p. Ablatio rechts St.p. 1x Lipofilling Mehrere Sitzungen notwendig Regelmäßige Sono + MRT Kontrollen Lipofilling + BRAVA • Roger Khouri ► Brustvergrößerung mit Eigenfett • ► Präoperative Expansion mit BRAVA – System • 10h pro Tag, mehrere Wochen • ► OP in Sedoanalgesie + LA • ► Injektionstechnik! • ► DISKUSSION: Mammographie – Kalzifikationen • ► 50 Patientinnen in 5 Jahren • ► sichere Methode • Lipofilling - Potentielle Risiken • Fettgewebsnekrosen • eventuelle Mikrokalzifizierungen • radiologische Fehldiagnostik • geringe Prädiktivität Lipofilling - Studie Vergleich der detektierten radiologischen Veränderungen nach verschiedenen Eingriffen an der Brust • • • • Mammareduktionen Mammarekonstruktionen Brusterhaltende OP Lipofilling Methodik - Radiologische Evaluation • Brustreduktion + Brustrekonstruktion + BET : • Sonographie: Vergleich prä- und postoperativ • Mammographie: Vergleich prä- und postoperativ • • MRT: bei unklaren Befunden • Biopsie: bei unklaren Befunden Methodik - Radiologische Evaluation Lipofilling • • • • • Sonographie: präop 1 Wo postop 1 Mo postop 4 Mo postop (präop 2. Sitzung) • • • Mammographie präop Patientinnen < Screeningalter: 12 Monate postop in 1 Ebene • • • Patientinnen > Screeningalter: 12 Monate postop in 2 Ebenen MRT: bei unklaren Befunden Biopsie: bei unklaren Befunden Methodik - Radiologische Evaluation • Fettgewebsnekrosen • (Mikro, Makrozysten, amorpher Kalk) • Mikrokalk • Architekturstörungen – Narbe • Karzinomverdächtige Veränderungen Methodik - Radiologische Evaluation n = 78 (53 Eingriffe Brust, 25 Lipofilling) Radiologische Veränderungen Nach Eingriffen an der Brust 24,5 % Karzinomverdächtige Veränderungen Lipofilling 32 % Nach Eingriffen an der Brust 0,53 % Lipofilling 0% Zukunft der Mammarekonstruktion • • • • Einfachere rekonstruktive Verfahren Patientenwunsch Zunahme der BET Nichtchirurgische Behandlung des Mammakarzinoms • Behandlung in Brustzentren Labien reduktions plastik syn: Labienkorrektur Labienreduktionsplastik Ursachen • konstitutionell, • Alter, • Multipara, • hormonell, • chronische Irritation (Manipulation, Geschlechtsverkehr, Entzündung), • Myelodysplastisches Syndrom (3) • Idiopathisch, … (1) Pardo et al.; International Journal of Gynecology and Obstetrics 2006; 93: 38 (2) Giraldo et al.; Plast Reconstr Surg 2004; 113: 1820 (3) Kato et al.; Urology 1988; 31: 294 Schamlippenverkleinerung Warum wünschen Frauen den Eingriff? - Unzufriedenheit mit dem Aussehen des äußeren Genitales (zu lange, unförmig, unsymmetrisch etc.) - Das äußere Genitale wird als „hässlich“ oder „Missbildung“ empfunden - Mentales Unwohlsein (best. Kleidung, öffentl. Bad, Sauna…) - Geschlechtsverkehr wird als unangenehm empfunden (emotionell & physisch) - Schmerz/Unwohlsein (Radfahren, Wandern u.a. Sportarten, Sitzen…) Labienreduktionsplastik Warum wünschen Frauen den Eingriff? Wichtige Zitate aus themenrelevanten Publikationen “ Although some women require surgical reduction for functional reasons, most seek size reduction of their labia minora because of psychological concerns.” (1) (1) Giraldo et al; Plast Reconstr Surg 2004; 113: 1820 Labienreduktionsplastik • Zentrale Resektion und Z- Plastik Labienreduktionsplastik • Tangentiale Resektion mit W - Plastik Labienreduktionsplastik • V- Exzision mit anteriorem Lappen Labienreduktionsplastik • Einfache Resektion Labienreduktionsplastik Amerika 2005 wurden 793 Eingriffe „vaginal rejuvenation“ 2006 Anstieg auf 1030 Eingriffe 0.08% aller kosmetischen Eingriffe Zunahme von etwa 30% (2005 2006) gehört die Labienreduktionsplastik jedoch zu den drei sich am schnellsten verbreitenden ästhetischen Eingriffen American Society of Plastic Surgeons “2006 Cosmetic Plastic Surgery Trends” . Assessed April 16, 2007 r Labienreduktionsplastik Die ausführliche Literature Recherche zeigt… Hypertrophie der labia minora ist selten. (1) Studien mit wenigen Patientinnen (2) nicht vergleichbar aufgrund unterschiedlicher Behandlungsmethoden. Das ästhetische Outcome wird in jeder Studie durch den/die behandelnden Chirurgen beurteilt. (1) (2) Rouzier et al.; Am J Obstet Gynecol 2000; 182: 35 Pardo et al.; Int J Gyn Obstet 2006; 93: 38-43 Labienreduktionsplastik - Ergebnisse - Zitate • Simple labial amputation „often results in a poor aesthetic outcome and sometimes even sexual dysfunction.“(1,2) • The amputation does not prevent postoperative discomfort and complications.“ (1) • „To achieve a perfect aesthetic result, the pigmented free edges of the labia minora must be preserved.“ (1) (1) (2) Rouzier et al.; Am J Obstet Gynecol 2000; 182: 35 Munhoz et al.; Plast Reconstr Surg 2006; 118: 1237 Labienreduktionsplastik Ergebnisse Zitate • Alter et al. 1998: • • Method: • („simple“) wedge resection • • • • Results and Complications: „minimal postoperative discomfort“ „well satisfied/pleased with the result“ „good postoperative result“ • The authors describe no complications n=4 follow up: ? Labienreduktionsplastik ErgebnisseZitate • • • • • • • • Giraldo et al. 2004: n=15 follow up: 30 mo. Method: wedge resection via „90-degree Z-plasty“ Results and Complications in 2 patients „minimal wound dehiscence“. All patients were fully satisfied with the aesthetic result All patients were satisfied with the functional result: problems of discomfort and anxiety had resolved, they felt greater self-esteem and confidence socially and in their personal relations. • The authors describe no complications Labienreduktionsplastik Ergebnisse Zitate • Rouzier et al. 2000: n=162 • follow up (clin.): 1 mo - 30 mo. • Method: • wedge resection via „inferior V-shaped resection“ • • • • • • • • • Results and Complications: Questionnaire (subjective): 89% satisfied with the aesthetic result 88% gained the aesthetic result they had expected 93% satisfied with the functional outcome 45% complained about postoperative discomfort, and 23% complained of entry dyspareunia for median 28 days 4% would not undergo the same procedure again. The authors describe no complications Labienreduktionsplastik Ergebnisse Zitate Maas et al. 2000: n=13 • • • Method: • wedge resection via „W-shaped resection“ • • • • • follow up: 2 mo. – 6 a Results and Complications: 11 patients „uneventful“ 1 patient: haematoma 1 patient: wound dehiscence „minimal postoperative discomfort“: pain for max. 2 we.; swelling for max. 4 we. • All patients: „Satisfactory Appearance“. • Postop., all patients were „pleased with the resolution of their original problems“ • The authors describe no complications Labienreduktionsplastik Ergebnisse Zitate • Choi et al. 2000: • • Method: • Excision of the central portion of the labium minus • • • • n=6 follow up: ? Results and Complications: All patients were satisfied with the functional outcome All patients were satisfied with the aestetic outcome „excellent aesthetic results“ • The authors describe no complications Labienreduktionsplastik Ergebnisse Zitate • Pardo et al. 2000: • • Method: • Laser labioplasty • • • • n=55 follow up: 2 mo. Results and Complications: 3 (5%): „minimal suture dehiscence“ 2 (4%): „mild to moderate pain“ within the first postop. week 50 (91%): very satisfied with aesthetic outcome, 5 pts (9%): satisfied • All patients: very satisfied with functional outcome • The authors describe no complications Labienreduktionsplastik Zusammenfassung • Verschiedene plastisch chirurgische Behandlungsmöglichkeiten • Prinzip: die pigmentierten freien Ränder der labia minora sollen bestmöglich erhalten werden • Verschiedene chir. Methoden mit gutem Outcome (subjektiv und klinisch) • Keine ernsten Komplikationen • Wesentlich ist: Erfahrung des behandelnden Chirurgen mit einer bestimmten OP-Methode Schamlippenverkleinerung Komplikationen • Sensibilitätsverlust • Verbreiterung, Bulging • Verschiebung der Grenze Haut/Mukosa • Verschiebung der Pigmentierung („Chessboard“) • Wundheilungsstörung • Narbenkontraktion • Verengung des Introitus vaginae • Verziehung der Harnröhrenöffnung Rechtliche Grundlagen • § 90 Abs 3 StGB bei Genitalverstümmelung Leitlinien Genitalchirurgie