P.Munda
Werbung

Leberzirrhose
ao. Univ. Prof. Dr. Petra Munda
Klinik f. Innere Medizin III
Abteilung f. Gastroenterologie und Hepatologie
Medizinische Universität Wien
Zirrhose
Endstadium jeder chron.
Lebererkrankung
Histologisch charakterisiert durch
Regeneratknoten und fibröses
Gewebe
Klinisch zwei Typen:
• kompensiert
• dekompensiert
Ursachen Zirrhose
Ursachen
•
•
•
•
•
•
•
•
•
•
Hepatitis B
Hepatitis C
Alkohol
NASH
PBC
AIH
PSC
Wilson
Hämochromatose
Alpha 1 AT-Mangel
Labormarker
• HBs-Ag, HBV-DNA
• HCV-Ak, HCV-RNA
• CDT, MCV, AST/ALT,
GGT
• AMA, SP-100
• ANA, ASMA, LKM, SLA
• ANCA
• Clp, 24hUCu, Genetik
• TFS%, Ferritin, Genetik
• Alpha 1 AT, Genetik
Natürlicher Verlauf chronischer
Lebererkrankungen
Chronic
liver
disease
Compensated
cirrhosis
Decompensated
cirrhosis
Entwicklung
von
Komplikationen
Varizenblutung
Ascites
Encephalopathie
Ikterus
Death
Entwicklung von Komplikationen
100
80
Ascites
Jaundice
Encephalopathy
GI
hemorrhage
Probability 60
of
developing 40
event
20
0
0
20
40
60
80
100
Months
Gines et. al., Hepatology 1987; 7:122
120
140
160
Dekompensation verkürzt das
Überleben!
100
80
Median survival
~ 9 years
All patients
with cirrhosis
60
Probability of
survival 40
20
Decompensated Median survival
~ 1.6 years
cirrhosis
0
0
20
40
60
80
100
Months
Gines et. al., Hepatology 1987;7:122
120
140
160
180
Leberzirrhose: Diagnose
Anamnese
Labor: Synthese, exkretorische Funktion
Ultraschall: Oberfläche, Lebervenen, Portalfluss
Histologie im Einzelfall
Schweregrad:
Child-Pugh Score (CPS)
MELD: 10 {0.957 Ln(Krea) + 0.378 Ln(Bili) + 1.12 Ln(INR) +
0.643}
Parameter
1 P.
2 P.
3 P.
Aszites
-
gering
ausgeprägt
Enzephalopathie
keine
I-II
III-IV
Serum-Bilirubin (mg/dl)
<2
2-3
>3
Normotest (%) (od EZ!)
>50
30-50
<30
Serum Albumin (g/dl)
>3,5
2,8-3,5
<2,8
Child Pugh A: 5-6 B: 7-9, C: 10-15
Laborparameter zur Diagnose
Normotest/PTZ ↓
Albumin ↓
CHE ↓
Thrombozyten ↓
Fibrinogen ↓ (Spätstadium)
Cholesterin ↓ (Spätstadium)
CT Scan in Cirrhosis
Liver with an irregular surface
Collaterals
Splenomegaly
Normal
Cirrhosis
Irregular surface
Nodules
GROSS IMAGE OF A CIRRHOTIC LIVER
Cirrhotic liver
Nodular, irregular surface
Nodules
Normal
Cirrhosis
Nodules surrounded
by fibrous tissue
HISTOLOGICAL IMAGE OF CIRRHOSIS
Fibrosis
Regenerati
ve nodule
Status bei Leberzirrhose
Lackzunge
Nabelhernie
Fehlende Behaarung
Aszites
Venenzeichnung
Spider naevus
IKTERUS
Dupuytren‘sche Kontraktur
Palmarerythem
COMPLICATIONS OF CIRRHOSIS
Komplikationen der Zirrhose resultieren
aus portaler Hypertension und/oder
Leberinsuffizienz!
Portale
Hypertension
Varizenblutung
Ascites
Zirrhose
Spontan
bakterielle
Peritonitis
Hepatorenales
Syndrom
Encephalopathie
Leber
insuffizienz
Ikterus
Portale Hypertension:
Diagnostik
Ultraschall
•
•
•
•
Zirrhose (höckrige Oberfläche)
Hepatofugaler Flow Pfortader
Splenomegalie
Rekanalisierte Umbilicalvene
Gastroskopie
• Varizen (Oesophagus, Fundus)
• Hypertensive Gastropathie
Lebervenendruckmessung
• Indirekte Portographie mit Ballonkatheter:
HVPG(Hepatic venous pressure gradient)
Portale Hypertension: Komplikationen
Varizenblutung
Aszites
Spontan bakterielle Peritonitis
Hepatische Enzephalopathie
Zirkulatorische Dysfunktion
Hepatorenales Syndrom
Hepatopulmonales Syndrom
VARICES INCREASE IN DIAMETER PROGRESSIVELY
Varices Increase in Diameter
Progressively
No varices
Small varices
7-8%/year
Merli et al. J Hepatol 2003;38:266
Large varices
7-8%/year
PROGNOSTIC INDICATORS OF FIRST VARICEAL HEMORRHAGE
Variceal hemorrhage
Varix with red signs
Predictors of hemorrhage:
Variceal size
Red signs
Child B/C
NIEC. N Engl J Med 1988; 319:983
ENDOSCOPIC IMAGES OF GASTRIC VARICES
Gastric Varices
Pretreatment
cyanoacrylate
Post-treatment
cyanoacrylate
Mild and Severe Portal Hypertensive Gastropathy
PORTAL HYPERTENSIVE
GASTROPATHIE (PHG)
Mild
Mosaic pattern
Severe
Mosaic pattern + red spots
Carpinelli et al. Ital J Gastroenterol Hepatol 1997; 29:533
Akute Varizenblutung-Managment
Konservative Transfusionspolitik (Hk 25 – 30 %)
Frühe Endoskopie (< 12 h)
Spezifische Therapie: *
• Medikamente: Terlipressin (TP), Somatostatin (SST)
• Endoskopische Behandlung
• Tamponade/ TIPS / Shunt-Chirugie
Prävention und Therapie der Komplikationen:
Infektionen
Enzephalopathie
Nierenversagen
Antibiotika
(Quinolone p. o.)
Magensonde,
Lactulose, LOLA
Hämodynamik,
NOR, Terlipressin
* Ziel: Blutungskontrolle und Prävention der frühen Rezidivblutung (5 d)
Sklerotherapie & Varizenligatur
Anwendungsbereich:
Sklerosierungsmittel:
v. a. Oesophagusvarizen
Äthoxysklerol
Varizenblutung
Basisdiagnostik Aszites
Anamnese
• kardial, hepatal, etc.
Status
• Flankenvorwölbung, Abdominelle Distension,
Nabelhernie, Dyspnoe
Diagnostik
• US
• Aszitespunktion (Parazentese)
Laborchemie (Zellzahl!)
Leuko>500/µl od Granulo>250/µl>SBP!)
Bakteriologie (cave kulturnegative SBP)
Zytologie (maligne Zellen?)
ASZITES THERAPIE
Unkomplizierter Aszites
• Salzrestriktion (2g/d)
• Diuretika (Spironolacton, Furosemid)
• Großvolumige Parazentese + Albumin
Refraktärer Aszites
• Großvolumige Parazentese + Albumin
• TIPS (transjugulärer intrahepatischer
portosystemischer Shunt)
THE TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
Transjugular Intrahepatic
Portosystemic Shunt
Hepatic
vein
TIPS
Portal vein
Splenic
vein
Superior
mesenteric vein
Pathogenese der HE:
Überblick
LeberNeurotoxische
insuffizienz
Portokavale
Umgehungskreisläufe
Störungen der Permeabilität
der Blut-Hirn-Schranke
Substanzen
(z.B. Ammoniak)
gelangen in
das Gehirn
Gliaschwellung Funktionsstörungen der Astroglia mit
Beeinträchtigung der
neuronalen Funktion
Änderungen intrazerebraler
Neurotransmitter (z.B. GABA)
und deren Rezeptoren
HE
Enzephalopathie: häufige
Auslöser
GI-Blutung
Infektion
Elektrolytstörung – Exsiccose
Diuretika
Diarrhoe
Emesis
Fieber
Sedativa
TIPS
STAGES OF HEPATIC ENCEPHALOPATHY
Stages of Hepatic Encephalopathy
Confusion
Drowsiness
Somnolence
Coma
1
2
Stage
3
4
HE: Klassifikationen
WCOG Wien 1998 Consensus, Hepatology 2002; 35: 716
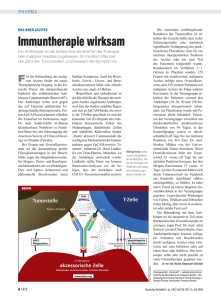
ASTERIXIS IS THE HALLMARK IN
THE DIAGNOSIS OF HE
Asterixis-Video
HEPATIC ENCEPHALOPATHY – TREATMENT SUMMARY
HE Therapie
Increase ammonia
fixation in liver:
Ornithine
aspartate
Benzoate
Shunt
occlusion
or
reduction
Decrease
ammonia
production in gut:
Lactulose
Antibiotics
Adjustment in
dietary protein
THERAPIE DER HE
oft reicht die Therapie des Auslösers!
Spezifische Therapie der akuten HE:
• L-Ornithin-L-Aspartat iv (Hepamerz®)
• Lactulose (Einlauf und/oder p.o.)
Rezidivprophylaxe:
• Rifaximin p.o. (Colidimin)
• L-Ornithin-L-Aspartat p.o. (Hepamerz®)
• Lactulose (mind 2 Stühle/d)
TAKE HOME MESSAGE
Leberzirrhose kann viele Jahre kompensiert
bleiben
Ab dem Zeitpunkt der ersten
Dekompensation beginnt die Uhr zu ticken!
Die Komplikationen (Varizenblutung,
Aszites, HE) sind zwar gut behandelbar,
verändern die Überlebenszeit aber nicht
wesentlich
Lebertransplantation ist die einzige kausale
Therapie