Prof. Dr. Reinier Mutters
Werbung

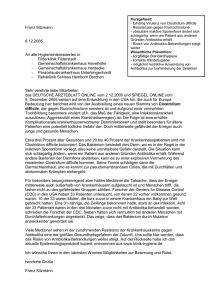
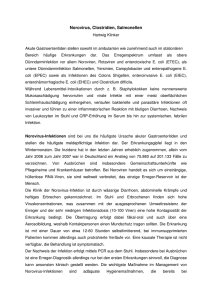
Prof. Dr. Reinier Mutters Institut für Medizinische Mikrobiologie und Krankenhaushygiene Philipps-Universität Marburg Universitätsklinikum Gießen und Marburg GmbH Bakterielle Darminfektionen • Peritonitis • Appendizitis • Enteritis – invasive (Ruhr-Typ) – nicht invasive (Cholera-Typ) Ursachen - Enteritis • Darminfektionen durch bakterielle Erreger meist durch Toxine bedingte Erkrankungen, oft im Zusammenhang mit der Aufnahme von Nahrungsmitteln. • Mit Infektion einhergehende Störung der Darmschleimhautfunktion führt zu Wasser- und Elektrolytverlust mit resultierender Dehydratation. • Häufige Symptome: – Übelkeit, Erbrechen, Durchfälle – (Fieber, Kopfschmerzen) Bakterielle Darminfektionen • invasive Enteritis (Ruhr-Typ) • • • • meist Dickdarm Erreger-Invasion in Darmwand Entzündung und Geschwürbildung blutige, schleimige Stühle Salmonellen Shigella Shiga-Toxin bildende E. coli EHEC Yersinia enterocolitica, Y. pseudotuberculosis Campylobacter jejuni Vibrio parahaemolyticus Clostridium difficile Bakterielle Darminfektionen • nicht invasive Enteritis (Cholera-Typ) • • • • Enterotoxinbildung im Dünndarm Sekretionsstörung Elektrolytverluste meist wässrige Durchfälle Vibrio cholerae Salmonellen Enterotoxin-bildende E. coli ETEC Enterotoxin-bildende Shigella dysenteriae Clostridium perfringens Clostridium difficile Bacillus cereus Staphylococcus aureus Bakterielle Darminfektionen Infektionsdosis • Salmonellen >1000 • Campylobacter <1000 • EHEC <100 • C. difficile 2 Diagnostik • Klinische Diagnostik • Mikrobiologische Diagnostik – auch weiterhin direkte und indirekte klassische Verfahren • kultureller Erregernachweis • ELISA • Immunoblot • Hämagglutination • sonstige Toxinnachweise • Agglutinationsverfahren zum Antigennachweis Diagnostik • Molekulare Verfahren wie die (Real Time) PCR finden langsam Einzug in die Diagnostik z.B. ETEC Enterotoxin-Nachweis, PCR-Nachweis von Salmomellen aus Lebensmitteln Aerobe gramnegative Erreger - Therapie 1 2 Salmonella 1,2 • Chinolone Gruppe 2 und 3 • (Co-trimoxazol) Æ Generierung von Dauerausscheidern nicht verhindert Yersinia 1 • Chinolon Gruppe 2 • (Co-trimoxazol) • (Tetracyclin) Campylobacter 1, einschließlich Arcobacter 1 • Clarithromycin • (Chinolon Gruppe 2) • (Tetracyclin) AB-Therapie bei schweren Formen mit Fieber, BK positiv, Patienten mit schweren Grunderkrankungen bei S. enterica ESBL nachgewiesen Hasman et al., J Antimicrob. Chemother. 56(1):115-121, 2005, Monno et al., Microb. Drug Res., 13(2), 124, 2007 Aerobe gramnegative Erreger - Therapie Shigella • Chinolon Gruppe 2 • (Co-trimoxazol) • (Ampicillin) Enteropathogene Escherichia coli (ETEC, EPEC, EIEC, EHEC) • • • • EHEC: Therapie mit Cotrimoxazol umstritten (Chinolon Gruppe 2 und 3) (Aminopenicillin/Betalaktamaseinhibitor) (Cephalsporin Gruppe 3) Aerobe gramnegative Erreger - Therapie • Providencia alcalifaciens (selten) • Ureidopenicillin • Cephalosporin Gruppe 3 • Chinolon Gruppe 2 Vibrio cholerae, Vibrio parahaemolyticus • Co-trimoxazol • Doxycyclin • (Chinolon Gruppe 2) Aerobe grampositive Erreger • Toxinbildende Staphylococcus aureus • Toxinbildende Bacillus cereus Anaerobier • Toxinbildende Clostridium perfringens • Toxinbildende Clostridium difficile Clostridium difficile C. difficile im Stuhl gesunde Erwachsene <3% gesunde Neugeborene 5 - 70% Kolonisation hospitalisierte Patienten 10 - 25% Acquisition von C. difficile im Krankenhaus: 13% bei Aufenthalt bis zu 2 Wochen 50% bei Aufenthalt >4 Wochen Schlottmann et al., Gastroenterologe 2:53 - 63, 2007 Barbut F, Petit J, Clin. Microbiol. Infect. 7: 405 - 410, 2001 Schröder, 2005 Clostridium difficile-associated Disease (CDAD) 1–2,5 % Letalität 30-Tage Letalität 6,1% Liegezeitverlängerung ITS 2,2 Tage Hospital 4,5 Tage Schröder, 2005; Keannelly et al., Chest 2007 Clostridium difficile O´Connor et al., Q J Med 97, 423-429, 2004 Clostridium difficile - Anstieg der Todesfälle in England und Wales Clostridium difficile-associated Disease (CDAD) Nosokomiale Infektion >70% der Fälle Verlängerter Krankenhausaufenthalt 8–36 Tage Zusätzliche Kosten pro Fall 6520 € Schlottmann et al., Gastroenterologe 2:53 - 63, 2007 Antibiotic associated diarrhea 2462 antibiotic-treated hospitalized patients 36% Cefpodoxime 26% Ceftazidime 25% Clindamycin 17% Cefotaxime 17% Quinolones (Ciprofloxacin) 7% Tetracycline Wistrom J JAC 47:43-50, 2001 Clostridium difficile - Antibiotika Antibiotic use in surgical patients with CDAD Ciprofloxacin, Cefoxitin, Cefepime, and Meropenem were the most commonly prescribed antibiotics before development of CDAD Patients with CDAD had higher mortality compared with control 31% vs. 11% (P =0.01) Average time from completion of antibiotic therapy to diagnosis was 7+2 days 16% developed CDAD after administration of prophylactic antibiotics Crabtree TD et al. Am Surg. 1999;65:507-512. Clostridium difficile Tasächliche Korrelation? Reflexion des Verschreibungsverhaltens (im ambulanten Bereich)? Loo et al., NEJM 353, 2442-9, 2005 Antibiotika und C. difficile • In keiner Studie – Angaben zu DD – Angaben zu individueller Medikation • Einfluss von AB nicht abzuschätzen • Wahrscheinlich: Alle AB, die Darmflora (Biotop) beeinflussen, relevant für C.diff-Infektion North American PFGE type 1 UK PCR ribotype 027 Toxinotype III Clostridium difficile NAP1/027/Tox III – Quebec/Montreal Quebec Inzidenz 22,5/1000 Einweisungen Letalität 6,9% >90 Jahre 74,4%/1000 Einweisungen Letalität 14% Erreger außerhalb Klinik: 33 Patienten 8 keine ABX 7 Infektion durch Kontaktperson Keine Risikopatienten Loo et al., NEJM 353, 2442-9, 2005 Chernak, Morbidity and Mortality Weekly Report 54: 1201-1205, 2005 Clostridium difficile – NAP1/027 Seit 2001 schwerwiegende CDAD-Fälle mit erhöhter Morbidität und Letalität USA Kanada UK Oktober 2001 März 2003 April 2003 300 Pat/12 Todesfällle (4%) Januar 2005 265/13 (4,9%) Juni 2005 565/25 (4,4%) Niederlande Juli 2005 Belgien Oktober 2005 Frankreich Juni-September 2006 Japan 10.1.2007 Erster Fall Kroatien 2007 Polen 2007 Österreich 2007 (1 Pat aus UK) Kanada Juni 2007: 53 Fälle/ 8 Todesfälle (15%) Æ 2000 Todesfälle durch NAP1 in Provinz Quebec seit 2003 Seit September 2007 in Deutschland Æ 1 Patient (NRW, Tourist aus Spanien) Trier 23 Patienten/9 Todesfälle Clostridium difficile - Eigenschaften • Erreger hochinfektiös und -kontagiös: Im Tiermodell genügte Inokulum von 2 Bakterien zum Auslösen einer Infektion • Ausscheidungsrate Patienten mit Diarrhöe 107 bis 109 Keime/g Stuhl Clostridium difficile McDonald et al., NEJM,353, 2005 Clostridium difficile – Häufigkeit Virulenzfaktoren (1) Meist: Toxin A- und Toxin B-positiv (2) Zunehmend: Toxin A-negative, Toxin B-positive Stämme, die typische CDADs verursachen (Toxinotyp VIII, Prävalenz in D 14,2%)* (3) Binäres Toxin bisher nur in Stämmen zu finden mit veränderten Toxin A- und Toxin B-Genen (Deletion im tcdA-Gen für Toxin A) (4) Toxin-Gene fehlen Æ apathogen, ohne klinische Bedeutung. Drudy et al., 2006, Alfa et al., 2000; Barbut et al., 2002; Stubbs et al., 2000; Rupnik, 2001 *European Study Group on Clostridium difficile (ESGCD), 16th ECCMID, Nizza 2006 Clostridium difficile NAP1/027 - Virulenzfaktoren Binäres Toxin 18 bp Deletion im tcdC-Gen (Negativ-Regulator der Produktion von Toxin A und B) Mutation in tcdC wahrscheinlicher Grund für Hyperproduktion der Toxine Æ 16 mal mehr Toxin A 23 mal mehr Toxin B Resistenz gegen Fluorchinolone und Cephalosporine Warny et al., 2005 Clostridium difficile – NAP1/027 Epidemischer Erreger mit veränderter Epidemiologie der CDAD Populationsgruppen mit zuvor geringem Risiko betroffen Æ Menschen jungen Alters gefährdet Fehlende vorherige Antibiotikatherapie schützt nicht vor CDAD CDADs nun auch außerhalb von Krankenhäusern Æ Surveillance-Studie Niederlande: 36% CDAD community-acquired Æ Ribotyp 027: Hinweis auf Zoonose Weitere Veränderungen: Blutige Durchfälle Hohe Rückfallraten Kuijper, E., 2006, Chernakl, E. et al., MMWR, 2005 C. difficile isolates from retail meats, United States Brandi Limbago, ICAAC 2007 Diagnostik: Clostridium difficile – Evolution of Testing Methods PCR ? Clostridium difficile - Direkter + indirekter Nachweis Toxine (A,B) Enzymimmunoassay RIDASCREEN© Clostridium difficile Toxin A/B (C0801) (R-Biopharm, Darmstadt) Immunchromatografischer Schnelltest remel x/pect® Clostridium difficile Toxin A/B Antigen (GDH) Enzymimmunoassay C. DIFF CHEK™-60 Antigennachweis - Glutamatdehydrogenase (Microtest, Mainz) Clostridium difficile - Probenhäufigkeit Nur EIA 72% (31/43) Æ Diagnose nach 1. Probe 84% (36/43) Æ Diagnose nach 2. Probe 93% (40/43) Æ Diagnose nach 3.Probe Konsequenz: "Cdiff 3 x Stuhl" Manabe Y. et al., Ann Intern. Med. 123:835-40, 1995 Clostridium difficile – Anaerobe Kultur Bei einem Ausbruch Evaluation einer neuen Test-Methode Surveillance von Antibiotika-Resistenzen Gelegentlich bei schwierigem Patienten-Management Zusätzliche Kultur bei negativem Toxin-Test erhöht Ausbeute (positiver Nachweis) um 15% - 23% Bouza, E. et al., J Hosp Infect 48:233, 2001 Reller, M.E. et al., J Clin Microbiol 2007 Clostridium difficile Primersequenzen für PCR, Real-Time PCR, TaqMan PCR Primer Nukleotidsequenz (5’-3’) Gene Fragmentlänge (bp) Referenz 16S rRNA 157 Rinttilä et al., 2004 tcdA441 TCTACCACTGAAGCATTA Toxin A 158 Bélanger et al., 2003 tcdA579 TAGGTACTGTAGGTTTATTG (tcdA) tcdB2667 ATATCAGAGACTGATGAG Toxin B 101 Bélanger et al., 2003 tcdB2746 TAGCATATTCAGAGAATATTGT (tcdB) cdtA-fw TGAACCTGGAAAAGGTGATG Binary Toxin 375 cdtA-rw AGGATTATTTACTGGACCATTTG (cdtA) cdtB-fw CTTAATGCAAGTAAATACTGAG (cdtB) cdtB-rw AACGGATCTCTTGCTTCAGTC (cdtB) Cdiff-fw TTGAGCGATTTACTTCGGTAAAGA Cdiff-rw CCATCCTGTACTGGCTCACCT 510 Terhes et al., 2004 HYGIENE - Clostridium difficile Übertragung Direkter Kontakt (Schmierkontamination) • in epidemischen Situationen USA: 30% der Hände von Mitarbeitern C. difficile-positiv • Persistenz durch Sporenbildung über längere Zeiträume (Wochen) Quantitative detection of Clostridium difficile in hospital environmental samples by real-time PCR Quantitative real-time PCR CDAD positive environment CDAD negative environment 1,E+05 CDAD positive environment CDAD negative environment 60 Q u a n ti fi c a ti o n 50 1,E+04 P e r c e n ta g e 40 30 20 1,E+03 10 0 1,E+02 Furniture Floor Toilet Hands Environmental samples Bedding Furniture Floor Toilet Hands Bedding Environmental samples CDAD negative environment = >6 Monate kein CD-Patient Mutters et al., 2008, submitted C. difficile – Hygienemaßnahmen Uniklinikum Marburg C. difficile ist ein hochgradig kontagiöser Erreger • Strikte Isolierung der Patienten • Patientenbezogene Nutzung von Medizinprodukten • Täglicher Wechsel der Bettwäsche, Transport/Aufbereitung als infektiöse Wäsche • Flächendesinfektion mit sporenwirksamen Mitteln (z.B. Perform®, Buraton®) • Schutzkittel, Handschuhe bei direktem Kontakt • erst Händedesinfektion • anschließend Händewaschen (Händesinfektionsmittel kaum sporenwirksam, Händedesinfektion zusätzlich wegen anderer enteraler Erreger) Therapie - Treatment of confirmed C. difficile infection • • First line: Metronidazol, oral – 500 mg/3x tgl oder 250 mg/4xtgl über 10 Tage – 9% Resistenz in Spanien (selten auch in Frankreich, UK) – bei NAP1 schlecht wirksam, hohe Rückfallquote (29%) Second line: Vancomycin, oral – 4 x 125 bis 500mg tgl. über 10 Tage – Vancomycin wegen • Schwangerschaft • Stillen • Metronidazol-Unverträglichkeit • Kein Ansprechen auf Metronidazol bach 3-5 Tagen Therapie – Risiko für VRE Norén et al., Antimicrob Ag. Chemother, 50: 3028-3032, 2006 Pelaez et al., Antimicrob Ag. Chemother, 46: 1647-1650, 2002 Bartlett JG. N Engl J Med. 2002;346:334-339 Wilcox, Kuiper, ICAAC 2007 Clostridium difficile – Antibiotika-Resistenz In vitro-Aktivität von Tigecyclin gegenüber Clostridium difficile Erreger Clostridium difficile (n=50) MHK-Bereich mg/l MHK50 mg/l MHK90 mg/l 0,016-0,032 0,032 0,032 Edlund C et al. Clin Microbiol Infect. 2000;6:158-163 Erreger MHK-Bereich MHK50 (µg/ml) MHK90 (µg/ml) Clostridium difficile ≤ 0,02 – 0,25 0,03 – 0,13 0,03 – 0,13 Noskin GA et al. Clin Infect Dis. 2005;41:303-314 Clostridium difficile – Antibiotika-Resistenz 110 toxinogene klinische Isolate (6 NAP1), isoliert 1983 - 2004 Antibiotikum MHK90 (µg/ml) Rifaximin 0,015 Rifalazil 0,03 Nitazoxanid 0,125 Tizoxanid 0,125 Hecht et al., Antimicrob Agents Chemother 51:2716-2719, 2007 Therapie Probiotika • Londoner Studie mit 135 einschließbaren Patienten • Drink mit: Lactobacillus casei, Streptococcus thermophilus, Lactobacillus bulgaricus 100g 2 x tgl. Alle erhielten 1 oder 2-3 Antibiotika 50% wg. Atemwegsinfekt, HWI, PAP (Aminopenicilline, Ceph1/2) Hochrisiko-AB ausgeschlossen Reduktion von AAD um 22% (95% CI 7%-37%, p=0,007) Reduktion von CDAD um 17% (95% CI 7%-27%, p=0,001) Hickson M. et al.: Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ. 2007 Jul 14;335(7610):80. Epub 2007 Jun 29 Alternativ-Therapie • Probiotische Joguhrt-Drinks senken CDAD-Risiko – Perenterol forte 250mg, tgl. 3x3 Kapseln (5,78€) – Hickson Actimel-Studie Pat./10Tage 14,80 € • Bei schwersten Verläufen oder toxischem Megakolon chirurgische Intervention erwägen "Actimel-Yacult"-Studie Teilnehmerrate: 6,8% Hickson M. et al. BMJ. 2007 Jul 14;335(7610):80 Therapie Probiotika zur Therapie bei oder Verhindern von Rezidiven Lactobacillus rhamnosus GG und Saccharomyces boulardii Lactobacillus casei, Streptococcus thermophilus, Lactobacillus bulgaricus Metaanalyse der heterogenen Studien: Zahlreiche offene Fragen Aufgrund des Risikopotentials ist Antibiotikatherapie zu bevorzugen Segarra-Newnham, Ann Pharmacother., 26.6.2007 (bisher nur epub)