Fieber - infekt.ch
Werbung

Infektiologische Notfälle
beim Erwachsenen in
der Praxis - ein Kroki
19. Infekttag 2014!
!
Carol Strahm!
Oberarzt // Klinik für Infektiologie & Spitalhygiene
Kantonsspital St. Gallen
Infektiologische Notfallkonsultationen: relevant?
15 Ärzte, 400 Notfallkonsultationen in der Schweiz
Prozent dringlicher Kons.
14-26%
HA vs Notfallarzt
345
55
Arbeitszeit vs Nacht
348
52
1. Platz: Obere Atemwegsinfekte!
2. Platz: Husten!
3. Platz: Fieber
Marty et al., PrimaryCare 2006;6: Nr. 18 // Evison et al., 2005, PMID 15999931 // Kwitkowski et al., 1999, PMID 10214210
Infektiologische NotfallInfektionen gehören zu häufigsten
konsultationen: relevant?
Noftallkonsultationen!
15 Ärzte, 400 Notfallkonsultationen in der Schweiz
meist relativ harmlose Infekte!
Prozent dringlicher Kons.
14-26%
Herausforderung !
HA vs Notfallarzt
345
55
Erkennen
des
wahren
Arbeitszeit vs Nacht
348
52
infektiologischen Notfalls!
ObereDiagnosen
Atemwegsinfekte!
auch 1.anPlatz:
seltene
denken!
2. Platz: Husten!Hospitalisation?
Notfall-Therapie,
3. Platz: Fieber
Marty et al., PrimaryCare 2006;6: Nr. 18 // Evison et al., 2005, PMID 15999931 // Kwitkowski et al., 1999, PMID 10214210
Infektiologischer Notfall
Infectious disease emergencies can be described
as infectious processes that, if not recognized
and treated immediately, can lead to significant
morbidity or mortality. These emergencies can
present as common or benign infections,
fooling the primary care provider into using
more conservative treatment strategies than are
required.
Kwitkowski et al., 1999, PMID 10214210
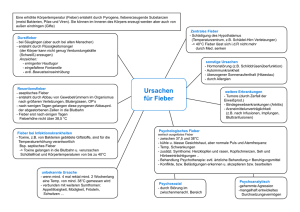
Beispiel: Sepsis
Üb
erl
ebe
n
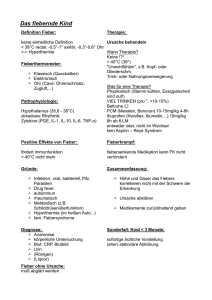
. Cumulative effective antimicrobial initiation following onset of septic shock-a
ion
and
survival. The x-axis represents time (hrs) following first documen
Kumar
et al.,associated
2006, PMID 16625125
Beispiel: Sepsis
Ü
ber
Empirische antibiotische
Therapie
leb
baldmöglichst und einnerhalb
1h
n
. Cumulative effective antimicrobial initiation following onset of septic shock-a
ion
and
survival. The x-axis represents time (hrs) following first documen
Kumar
et al.,associated
2006, PMID 16625125
ock.7’2
e
An additional
application
to
source
of the
of confusion
terms
noninfectious
sepsis
and
inflammatory
has
states.
13.14
simplification
of this
these
processes,
recommendations
d
o compare
blood cell count,
such as a count
cu mm, a count less than 4,000/cu
to
of
is necessary
and
for both
clini-
sepsis
and its sesuch as sepsis,
the
evaluate
s
is significantly
should be used
of
future
investigations
into
and treatment
modalities.
therapeutic
new
this
response
inflammatory
variety
the phrase
syndrome
(SIRS)
process,
independent
(Fig 1).
systemic
inflammatory
a wide
propose
to
of
of insults
and
can
be
includes,
seen
but
is
than
than 90
by a
minute,
greater
than 12,000/
mm, or the presence
immature
changes
neutrophils
should
from baseline
in the
for such abnormalities,
induced
neutropenia,
systemic
with
and
represent
absence
such
leukopenia.
inflammatory
a large
number
response
is
of clinical
Besides
the infectious
insults
that
SIRS,
noninfectious
pathologic
causes
pancreatitis,
injury,
ischemia,
hemorrhagic
multiple
shock,
of
as
may
may
trauma
and
immune-mediated
organ injury, and the exogenous
administration
of such
putative
mediators
of the inflammatory
process
as
tumor
necrosis
factor
and other
cytokines.
A frequent
complication
ofSIRS
is the development
of organ
system
dysfunction,
including
such
welldefined
renal
response
percent
physiologic
Rationale:
The
seen
in association
tissue
We therefore
10
These
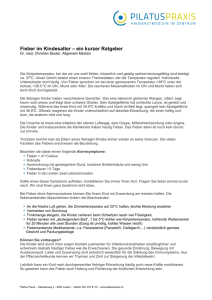
Definition SIRS und Sepsis!
clinical
greater
as indicated
by a PaCO2 of less
and (4) an alteration
in the white
an acute
alteration
other
known
causes
include
erm sepsi
in popular
usage,
implies
a clinical
arising
from infection.
It is apparent
that a
or even
identical,
response
can arise
in the
ofinfection.
inflammatory
than
conditions.
produce
1
tion
more
chemotherapy,
improved.
The following
as general
guidelines
in the
potential
or hyperventilation,
than
32 mm Hg;
(“bands”).
following
than 36#{176}C;
(2) a heart rate greater
minute;
(3) tachypnea,
manifested
rate greater
than
20 breaths
per
of
concerning
terms,
protocols
38#{176}Cor less
of the
temperature
this consensus
conference
for the standardization
in communication
researchers
By standardizing
one
To
of terminology
confusion
than
(1) a body
termino1ogy’3” ’7
.
tandardization
to, more
beats
per
respiratory
editorials
and position
papers
have recently
to provide
a framework
for the standardi-
nd
not limited
manifestations:
septic
clinical
failure,
conditions
and
as acute
multiple
drome
(MODS).
The
consensus
conference,
organ
lung
injury,
shock,
dysfunction
term MODS
also stems from
and its definition
will be
synthis
dis-
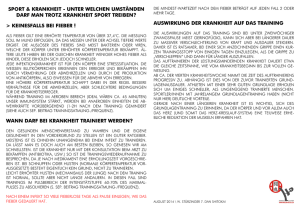
Körpertemperatur > 38 °C oder < 36 °C
Tachykardie: Herzfrequenz > 90/min
Tachypnoe: Atemfrequenz > 20/min oder
Hyperventilation (PaCO2 < 4,3 kPa)
Leukozytose (> 12/G/l) oder Leukopenie (< 4/
G/l) oder > 10 % Linksverschiebung
2 Kriterien für SIRS
BLOOD
FIGURE
1. The
interrelationship
BORNE
between
systemic
INFECTION
inflammatory
response
syndrome
(SIRS),
sepsis,
and
infection.
CHEST
urnal.publications.chestnet.org/ on 02/24/2014
I 101
I 6 I JUNE,
1992
1645
Sepsis: SIRS durch Infektion
Bone et al., 1992, PMID 1597042 // Levy et al., 2003, PMID 12664219
ock.7’2
e
An additional
application
to
source
of the
of confusion
terms
noninfectious
sepsis
and
inflammatory
has
states.
13.14
simplification
of this
these
processes,
recommendations
d
o compare
blood cell count,
such as a count
cu mm, a count less than 4,000/cu
to
of
is necessary
and
for both
evaluate
is significantly
should be used
of
future
investigations
into
and treatment
modalities.
improved.
The following
as general
guidelines
in the
potential
response
inflammatory
new
conditions.
produce
a wide
variety
the phrase
syndrome
(SIRS)
process,
independent
(Fig 1).
systemic
inflammatory
of insults
and
than 90
by a
minute,
greater
than 12,000/
mm, or the presence
immature
changes
neutrophils
should
from baseline
in the
for such abnormalities,
represent
absence
such
of
as
to
of
can
be
includes,
seen
but
is
induced
neutropenia,
systemic
with
and
leukopenia.
Körpertemperatur > 38 °C oder < 36 °C
inflammatory
a large
number
response
is
of clinical
Besides
the infectious
insults
that
SIRS,
noninfectious
pathologic
causes
pancreatitis,
injury,
ischemia,
hemorrhagic
multiple
shock,
may
may
trauma
and
immune-mediated
organ injury, and the exogenous
administration
of such
putative
mediators
of the inflammatory
process
as
tumor
necrosis
factor
and other
cytokines.
A frequent
complication
ofSIRS
is the development
of organ
system
dysfunction,
including
such
welldefined
renal
response
percent
physiologic
Rationale:
The
seen
in association
tissue
propose
10
These
than
as indicated
by a PaCO2 of less
and (4) an alteration
in the white
an acute
alteration
other
known
causes
include
We therefore
than
chemotherapy,
erm sepsi
in popular
usage,
implies
a clinical
arising
from infection.
It is apparent
that a
or even
identical,
response
can arise
in the
this
more
Definition SIRS und Sepsis!
clinical
greater
SIRS (zu) Tachykardie:
sensitiv,Herzfrequenz
unspezifisch!!
> 90/min
Tachypnoe:
Atemfrequenz > bewiesen
20/min oder
Sepsis oft erst
retrospektiv
therapeutic
1
ofinfection.
inflammatory
or hyperventilation,
than
32 mm Hg;
(“bands”).
sepsis
and its sesuch as sepsis,
the
s
tion
clini-
following
than 36#{176}C;
(2) a heart rate greater
minute;
(3) tachypnea,
manifested
rate greater
than
20 breaths
per
of
concerning
terms,
protocols
38#{176}Cor less
of the
temperature
this consensus
conference
for the standardization
in communication
researchers
By standardizing
one
To
of terminology
confusion
than
(1) a body
termino1ogy’3” ’7
.
tandardization
to, more
beats
per
respiratory
editorials
and position
papers
have recently
to provide
a framework
for the standardi-
nd
not limited
manifestations:
septic
clinical
failure,
conditions
and
as acute
multiple
drome
(MODS).
The
consensus
conference,
organ
lung
injury,
shock,
dysfunction
term MODS
also stems from
and its definition
will be
syn-
this
dis-
Hyperventilation (PaCO2 < 4,3 kPa)
Leukozytose (> 12/G/l) oder Leukopenie (< 4/
G/l) oder > 10 % Linksverschiebung
2 Kriterien für SIRS
BLOOD
FIGURE
1. The
interrelationship
BORNE
between
systemic
INFECTION
inflammatory
response
syndrome
(SIRS),
sepsis,
and
infection.
CHEST
urnal.publications.chestnet.org/ on 02/24/2014
I 101
I 6 I JUNE,
1992
1645
Sepsis: SIRS durch Infektion
Bone et al., 1992, PMID 1597042 // Levy et al., 2003, PMID 12664219
Frage: Erkennung des infektiologischen Notfalls? Was hilft am
wenigsten … ?
1. Vitalparameter (Fieber, BD, Puls,
Atemfrequenz)!
2. Klinische Untersuchung!
3. Anamnese (Jetziges Leiden)!
4. Laborparameter!
5. Persönliche Anamnese
Biomarker bei akuten Infekt
Simon et al., 2004, PMID 15307030 // Lee et al., 2012, PMID 21514766 // Selberg et al., 2000, PMID 10966252
CRP kann nicht unterscheiden zwischen:
- SIRS und Sepsis!
Biomarker bei akuten Infekt
- Bakteriämie und keine Bakteriämie (Infekt)!
- Infekt vs kein Infekt (insbesondere <12h)
Simon et al., 2004, PMID 15307030 // Lee et al., 2012, PMID 21514766 // Selberg et al., 2000, PMID 10966252
Wichtigste Warn- und
Leitsymptome
Bei welchen Symptomen muss man sofort
handeln?
Wichtigstes Leitsymptom: Akutes
Fieber beim Erwachsenen
Fieber (insbesondere >39°C) selten beim Erwachsenen,
wichtigstes Warnsymptom für eine bakterielle
Infektion!
im Gegensatz zu Kindern!
Cave: ältere Menschen (Hypothermie!), Steroide, NSAR!
andere Differentialdiagnosen!
Influenza!
nicht-infektiös: maligne Hyperthermie, malignes
Neuroleptika-Syndrom, Medikamentenfieber, zentrales
Fieber, rheumatologische Erkrankungen, …
Evison et al., 2005, PMID 15999931 // Lee et al., 2012, PMID 21514766 // Lee et al., 2012 PMID 22463870
Akutes hohes Fieber
Vitalparameter sorgfältig messen, Verlauf? (Hf, AF, BD)!
Anamnese!
Chronische Erkrankungen (Diabetes mellitus, Hämodialyse,
Zirrhose, Tumor, …); Asplenie, Immunsupression, Chemotherapie!
Reiseanamnese, Tiere, Beruf, Hobbies, Sexualanamnese!
zusätzliche Symptome (Schüttelfrost, Husten, Halsschmerzen,
Gelenkschmerzen, Kopfschmerzen, …)!
Status mit Frage nach Infektfokus (Meningismus, Lunge,
Abdomen, Haut, Nierenlogen, …)!
Zeichen des Organversagen? Respiratorisches Versagen,
Desorientiertheit, Hypotension, Gerinnungsstörung!
Labor notwendig? BB mit Diff, CRP, Leberwerte, UST, Kulturen, ….
Sofortige Antibiotikatherapie?!
Rasche Hospitalisation?
Fieber + Schüttelfrost
,shaking chills’od. ‚rigor‘
Pyrogene Cytokine verändern ‚Setpoint‘ im
Hypothalamus und können so Schüttelfrost auslösen!
no - mild - moderate - shaking chills!
1/3 der Patienten mit ‚Shaking chills‘ hatten
Bakteriämie, fast 50% der Patienten mit Bakteriämie
hatten ‚Shaking chills‘!
je schwerer Schüttelfrost desto spezifischer für
Bakteriämie!
‚Chills‘ allgemein Sens. und Spez. ca 60-70%, besseres
long-term survival?!
DD Medikamente, Blutprodukte, …
Evison et al., 2005, PMID 15999931 // vanDissel et al., 1998, PMID 9717936 // Holtzclaw, 2004, PMID 15461043// Tokuda et al., 2005, PMID
16378800 // vanDissel et al., 2005, PMID 15836664 // Lee et al., 2012, PMID 22463870
Fieber + Schüttelfrost
,shaking chills’od. ‚rigor‘
Pyrogene Cytokine verändern
‚Setpoint‘ im
Echter Schüttelfrost
ist
guter
Hypothalamus und können so Schüttelfrost auslösen!
Hinweis für
eine
Bakteriämie
und
no - mild
- moderate
- shaking chills!
1/3 der Patienten mit ‚Shaking chills‘ hatten
sollte bei Fieber
und
Infektverdacht
Bakteriämie, fast 50% der Patienten mit Bakteriämie
hatten ‚Shaking chills‘!
immer erfragt werden!!
je schwerer Schüttelfrost desto spezifischer für
Bakteriämie!
WARNSYMPTOM
für Sepsis
‚Chills‘ allgemein Sens. und Spez. ca 60-70%, besseres
long-term survival?!
DD Medikamente, Blutprodukte, …
Evison et al., 2005, PMID 15999931 // vanDissel et al., 1998, PMID 9717936 // Holtzclaw, 2004, PMID 15461043// Tokuda et al., 2005, PMID
16378800 // vanDissel et al., 2005, PMID 15836664 // Lee et al., 2012, PMID 22463870
Frage: Haben sie Rocephin®
(Ceftriaxone) in der Praxis?
1. ja, habe es aber noch nie verwendet!
2. ja, habe es in Notfallsituationen auch
schon verwendet!
3. nein, weil meine Praxis nahe an einem
(Zentrums)spital ist!
4. nein!
5. nein, ich habe prinzipiell keine IV
Medikamente
Wann empirische antibiotische
Therapie in der Praxis?
nie bei Protheseninfektionen und fremdkörperassoziierten Infekten, Endokarditis, Abszessen etc!
bei stabilen Patienten möglichst rasche
Hospitalisation anstreben!
Indikationen (falls Hospitalisationsweg >1h)!
Verdacht auf (Meningokokken)meningitis!
Infekt beim asplenischen Patienten!
septisch-toxischer Schock!
möglichst immer vorher 2x2 Blutkulturen!
Evison et al., 2005, PMID 15999931
Fieber + Hypotonie/ AZVerschlechterung
rasche AZ Verschlechterung / Fieber PLUS Hypotonie
(Systolischer BD <90mmHg), Tachycardie, erhöhte Atemfrequenz
hoher Verdacht auf SEPSIS (Infektiologischer Notfall)
Hypotonie im Rahmen einer Sepsis: Empirische
Antibiotikatherapie und Sepsistherapie (Volumen, etc) spätestens
innerhalb einer Stunde!
Organversagen? Verwirrung, Eintrübung, Dyspnö, …!
Häufigste Infektfoci:!
Lunge (Pneumonie, Empyem); Abdomen (Cholangitis, Peritonitis,
Perforationen, Abszesse); Harnwege (Pyelonephritis); Haut
(Cellulitis, …)!
,Toxic Shock Syndrome’
Evison et al., 2005, PMID 15999931
‚Toxic Shock
Syndrome‘ (TSS)
Infektion mit Staphylococcus aureus oder Gruppe-A-Strepotokokken
(GAS, S. pyogenes)!
Infektfokus klinisch nicht im Vordergrund, primär toxin-vermittelte
Erkrankung die früh mit Schock und Multiorganversagen verläuft!
Erythrodermie, Organbeteiligung (Diarrhö, Erbrechen, Verwirrtheit,
Niereninsuffizienz, Konjunktivitis, …)!
Staphylococcus aureus!
menstruales TSS: vor allem in der 80er Jahren bei Frauen in
Zusammenhang mit Tampons, in letzter Zeit eher wieder zunehmend!
nicht-menstruales STSS: häufiger!
Streptococcus pyogenes (GAS)!
sekundär zu invasiven GAS-Infektionen (Tonsillitis bis
nekrotisierende Fasziitis)
Evison et al., 2005, PMID 15999931 // Lappin et al., 2009. PMID 19393958
‚Toxic shock syndrome‘
•
•
•
•
•
sofortige Hospitalisation!
Floxapen PLUS Clindamycin!
Infektsanierung!
eventuell IVIG!
Dekolonisierung
‚Toxic shock syndrome‘
Fieber + Hautausschlag und
Petechien
Fieber, AZ-Verschlechterung und rasch auftretende
Effloreszenzen (va Exanthem -> Petechien)!
Petechien: Prädilektionsstellen sind Handgelenke, Knöchel,
Axillae, enorale Schleimhäute, Konjunktiven und Druckstellen im
Bereich der Kleider!
Warnsymptom für!
Disseminierte intravasale Gerinnung (DIC)!
septische Embolie: Schmerzhafte „Knoten“ an Akren / SplinterHämorrhagien!
Vaskulitis!
Infektiologische DD: Meningokokken(meningitis), Endokarditis,
schwere Sepsis (gramnegative Sepsis, Capnocytophaga canimorsus),
hämorrhagisches Fieber, Rickettsiosen
Evison et al., 2005, PMID 15999931
Meningokokkenmeningitis
Fieber + Verwirrtheit und
Kopfschmerzen
Fieber mit neu aufgetretenen ZNS-Symptomen: typisches
Zeichen für Meningitis und Enzephalitis !
Verwirrtheit!
Bewusstseinsstörungen!
Kopfschmerzen!
Meningismus (kann insbesondere bei älteren Patienten fehlen)!
bei älteren Patient mit Verwirrtheit an (schweren) Sepsis mit
Organdysfunktion denken!
Krampfanfälle, fokale neurologische Ausfälle: Enzephalitis?!
Herpes simplex Virus Enzephalitis (meist ohne Effloreszenzen),
rasche antivirale Therapie! und FSME (Impfung!)
Evison et al., 2005, PMID 15999931
Bakterielle Meningitis
Fieber, Kopfschmerzen, Meningismus, Bewusstseinsstörung; >95% mind 2/4 Symptome!
Erbrechen, Rückenschmerzen, Myalgien, Exanthem,
Otitis, Photophobie, Krampfanfall!
Für Prognose: rasche antibiotische Therapie: Ziel
innerhalb 1h (ZNA innerhalb 15 Minuten), Steroide!
schlechte Prognose: Alter, Organversagen,
Bewusstseinsveränderungen, Krampfanfälle,
Symptome >24h!
Procedere: 2x2 BK, 10 mg Dexamethason, Rocephin 2g
IV, ev Amoxicillin, LP (allenfalls vorher CT Schädel)
Evison et al., 2005, PMID 15999931 // Aronin et al., 1998, PMID 9867727 // Kwitkowski et al., 1999, PMID 10214210 // van de Beek et al.,
2004, PMID 15509818 // Vibha et al., 2010, PMID 20577910
Fieber + Muskelschmerzen
kann Hinweis auf eine Myalgie im Rahmen einer
disseminierten bakteriellen Infektion sein!
Lokalisation vor allem im Rücken und Waden!
vor allem bei Meningokokken, Staphylokokken und
Streptokokken!
Pyomyositis mit/ohne Abszess vor allem Psoas zum
Beispiel Staphylococcus aureus!
Starke Schmerzen in Extremitäten relativ
unauffälligem Lokalbefund: nekrotisierende
Fasziitis
Evison et al., 2005, PMID 15999931
Nekrotisierende Fasziitis:
Klinische Alarmzeichen
Massivste Schmerzen bei Schwellung mit nur wenig
Rötung: ‚Pain out of proportion‘!
Schnelle Progredienz (Bullae, Nekrosen, Gasbildung)!
Unruhe, Delir, Fieber!
Tachykardie, Hypotonie, toxischer Schock!
!
Therapie !
Chirurgie ist vordringlich!
Augmentin plus Dalacin (falls community acquired),
Imipenem plus Dalacin (falls multimorbid, Auftreten
postoperativ, v.a. nach Bauchoperationen)
Nekrotisierende Fasziitis
Fieber + Husten und
Dyspnö
Fieber + Neutropenie
Fieber (>38.3 einmalig oder zweimal >38°C
innerhalb einer Stunde) beim neutropenen Patienten
(<500 Neutrophile) ist ein infektiologischer Notfall!
signifikant höheres Risiko für fulminant verlaufende
Infektionen durch grampositive und gramnegative
Erreger sowie Candidainfektionen!
Risiko steigt je nach Schweregrad der Neutropenie
(Hochrisiko < 100) und Dauer (>10 Tage)!
oft zeigt sich klinisch kein Infektfokus!
rasche Hospitalisation für Diagnostik und Therapie
Evison et al., 2005, PMID 15999931 // de Naurois et al., 2010, PMID 20555092 // Freifeld et al., 2011, PMID 21205990
Fieber + Immunsuppression
Patienten mit immunsuppressiver Therapie!
Tumoren, Leukämie, Transplantation,
Autoimmunerkrankungen
Rheumatologische Patienten!
Symptome
Normaler Patient
Biologicals (TNFalpha Blocker); Cytotoxische
Medikamente (MTX, AZT, ..), Steroide!
häufiger bakterielle Infekte (Pneumonien),
häufigster Opportunist: PCP; TNFalpha
Blocker: TBC!
Tansplantierte Patienten!
Fieberursachen: Infekte, Abstossung,
Drugfever, Autoimmunerkrankungen!
Immunsupprimierter
Patient
Typische ‚Timeline‘ der Infektionen; ‚net state
of immunosuppression‘ und
Expositionsrisiko!
Zeit
cave Interaktionen von Antibiotika
(Makrolide, Chinolone, Sulfonamide)
Evison et al., 2005, PMID 15999931 // dePeddi, et al., 1997, PMID 9167657 // Greenberg, 2002, PMID 12418448 // PG Course
Fieber + Asplenie
Fieber bei funktioneller (Sichelzellanämie, Hb-Pathien)
oder anatomischer Asplenie ist immer Warnzeichen für
ein OPSI (overwhelming postsplenectomy infection)!
Inzidenz 0.23%/y, Lifetime-Risk ca 5%!
Mortalität 50-70%, frühe Therapie 10-40%!
initial oft Grippe-Symtome, rasch schwere Sepsis
(Klinik wie Meningokokkenmeningitis mit DIC)!
Erreger: Pneumokokken > Meningokokken > H. influenzae;
Capnocytophaga canimorsus (Hundebiss!), Malaria!
Splenektomieausweis und Patientenaufklärung sehr
wichtig, aber: Patiententen sind oft nicht informiert
Evison et al., 2005, PMID 15999931 // Morgan et al., 2012, PMID 22726665 // Waghorn et al., 1997, PMID 9459404
Fieber + Asplenie
Fieber bei funktioneller (Sichelzellanämie, Hb-Pathien)
oder anatomischer Asplenie ist immer Warnzeichen für
ein OPSI (overwhelming postsplenectomy infection)!
Inzidenz 0.23%/y, Lifetime-Risk ca 5%!
sofortige Zuweisung Notfall und
initial oft Grippe-Symtome, rasch schwere Sepsis
(Klinik wie Meningokokkenmeningitis
mit DIC)!IV)
antibiotische Therapie
(zB Rocephin
Mortalität 50-70%, frühe Therapie 10-40%!
Erreger: Pneumokokken > Meningokokken > H. influenzae;
Capnocytophaga canimorsus (Hundebiss!), Malaria!
Splenektomieausweis und Patientenaufklärung sehr
wichtig, aber: Patiententen sind oft nicht informiert
Evison et al., 2005, PMID 15999931 // Morgan et al., 2012, PMID 22726665 // Waghorn et al., 1997, PMID 9459404
Fieber + ein geschwollenes
Gelenk: septische Arthritis
seltene Erkrankung: Inzidenz ca 4-10/100000 (EU)!
Inzidenz eher zunehmend (zunehmendes Alter,
Immunsuppression, invasive Eingriffe, Prothesen!!)!
Systemische Symptome: selten!!
34% Fieber; 15% Schwitzen; 6% Schüttelfrost!
lokale Rötung, Schwellung, Erguss, Schmerzen!
meist grosse Gelenke (Knie!), 20% Polyarthrikulär!
case fatality rate ca 11%!
Abgrenzung zur Kristallarthropathie nur durch Punktion
möglich!
CAVE: Prothesengelenke nicht in der Praxis punktieren
Mathews et al., 2010, PMID 20206778
Fieber + ein geschwollenes
Gelenk: septische Arthritis
seltene Erkrankung: Inzidenz ca 4-10/100000 (EU)!
AB Therapie erst nach Diagnostik!!
Inzidenz eher zunehmend (zunehmendes Alter,
Immunsuppression, invasive Eingriffe, Prothesen!!)!
!
Systemische Symptome: selten!!
Septische Arthritis ist dringliche bis
notfallmässige
meist grosseOperationsindikation!
Gelenke (Knie!), 20% Polyarthrikulär!
34% Fieber; 15% Schwitzen; 6% Schüttelfrost!
lokale Rötung, Schwellung, Erguss, Schmerzen!
case fatality rate ca 11%!
Abgrenzung zur Kristallarthropathie nur durch Punktion
möglich!
CAVE: Prothesengelenke nicht in der Praxis punktieren
Mathews et al., 2010, PMID 20206778
Fieber + Halsschmerzen
meist Pharyngotonsillitis!
50-80% virale Infekte; Therapie nur Gruppe A
Streptokokken 15-20%!
DD STD (HIV, Lues, Gonorrhoe)!
Sehr starke Schmerzen, Halsschwellung, hohes
Fieber!
bakterieller Infekt mit Abszedierung
(Peritonsillarabszess, Retropharyngealer Abszess,
Zungengrundabszess)!
Inspiratorischer Stridor: akute Epiglottitis
Evison et al., 2005, PMID 15999931
Fieber + Halsschmerzen
HIV!
meist Pharyngotonsillitis!
Primoinfekt!
50-80% virale Infekte; Therapie nur
Gruppe A
Streptokokken 15-20%!
DD STD (HIV, Lues, Gonorrhoe)!
Sehr starke Schmerzen, Halsschwellung, hohes
Fieber!
bakterieller Infekt mit Abszedierung
(Peritonsillarabszess, Retropharyngealer Abszess,
Zungengrundabszess)!
Inspiratorischer Stridor: akute Epiglottitis
Evison et al., 2005, PMID 15999931
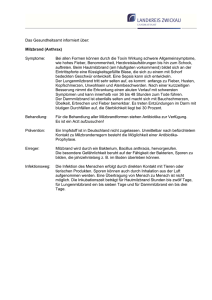
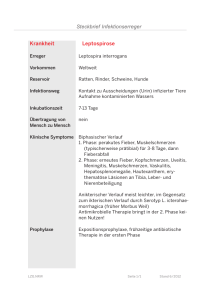
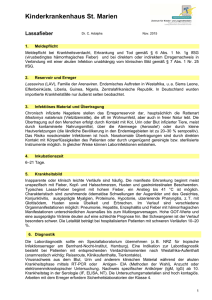
Fieber + Reiserückkehrer
Bedrohlichkeit!
Häufigkeit!
Meningitis
Viral. hämor. Fieber Malaria
Typhus abdominalis
Amöben-Leberabszess
Urosepsis
Pneumonie
Dengue-Fieber
Diarrhöe!
Atemwegserkrankungen
Diarrhöe
Hautinfekte
Dengue
Urosepsis
Malaria
Typhus abdominalis
Meningitis!
Hatz, Schweizerisches Tropeninstitut // Bertisch et al., 2012, Swiss Medical Forum // Nilles et al., 2012, PMID 21908138
5N6:E%JN8#JE%6K%8J%38%J J%3J377N8#%)T3%8K%8J2
K3%8K%8?AJ%3JN((663-5%3K%8J(:6-KJ#3%J8K%DEN 1N8-J#%EJ
:D-%8E=NKN7EJP:8J#D%3JN(%388#%D(:6-%8#%8J-%8J
>--(AJ=D:P:T3%DK?AJ38J
2%EKJ3EKJ%3JN%D5N6:E%J377%DJ
38#3T3%DKJMLAJ%D#%J%3J3-D8K%8J73KJ(DO1%D%DJN%D2
5N6:E%%18#6N8-J :#%DJ %D5N8(KJ NEJ : 1=DP6%8T2
68#%D8J3EKJ%38%J%E3EK%8TK%EKN8-J%D(:D#%D63 1JN8#J#3%J
%18#6N8-J73KJ%38%7J=%T363EK%8JTNJ%E=D% 1%8JMUAJ
:DJ-%=68K%DJ
77N8EN==D%EE3:8J3EKJ%38%J6K%8K%JN%D2
K%D%8J1D%8JN 1J(ODJK3%8K%8JNEJE3%8JN8#JO#%N2
D:=JMMJK3%(%D%J,2%DK%J%3J38KD3KKJ6EJ%3J 1Q%32
T%D8AJ5KN%66%JK%8JT%3-%8J%38%J%D1;1K%JDN 1DK%J
#%DJ8K3D%KD:P3D6%8J1%D=3%J>?J%3J23-D8K%8J
MM"JL<AJ%3J%DO 5E3 1K3-N8-JP:8J:D%18#6N8-"J%2
E3EK%8T6-%J N8#J %8:KS=J 3EKJ #EJ 8E=D% 1%8J N(J #3%J
1%D=3%J83 1KJ%%38KD 1K3-KJLMAJ%3J23-D8K%8J
38J #%DJ J (8#J E3 1J 5%38%J Q%3 1N8-J %TO-63 1J
:DK63KKJ:#%DJ
2K%JL<AJ
Fieber + Reiserückkehrer
Bedrohlichkeit!
Meningitis
Viral. hämor.
Fieber .?3<&!
?3<&!<+:<10=!
!)9!9!<10=!
3(H -. >
Malaria
,.0H3(H3N-. >
Typhus abdominalis
0HE D-3# 0E.53
.>1 D,25>>,(.?, D. >
Amöben-Leberabszess
N8,H?
Urosepsis
1>.D9<D#1.8>H2: und meist 10d bis 4 Wochen
1>.D9<DK.KMD5K1 D21>. :
Pneumonie
H >0H15?
Dengue-Fieber
>H 115?
8E.E.?DD Diarrhöe!
!--!<>
30HE.53?O .E 3D9, 111H:DH3D26(1., D ?,L > 38 >?.?E 3OD9H30 11H:<D
Häufigkeit!
Atemwegserkrankungen
)9!Diarrhöe
Hautinfekte
Dengue
Urosepsis
Malaria
Typhus abdominalis
Meningitis!
8E.E.?DD
.?O >1 D .?,23.5?
.1>.5? 3
,.?E5?52.?.?D9,>53.?, ?D
E.H2:
26 31 >?O ??D
Hatz, Schweizerisches Tropeninstitut // Bertisch et al., 2012, Swiss Medical Forum // Nilles et al., 2012, PMID 21908138
Fieber + Reiserückkehrer
nach Tropen: immer Malaria ausschliessen!!
Symptome unspezifisch: Fieber, Kopfschmerzen und
Malaise am häufigsten !
Reiseort und Zeit? Malariarisiko? Wurde Prophylaxe
genommen? Moskito-Schutz? (Subsahara-Afrika höchstes Risiko)!
3x dicker Tropfen (febril, 12-24h Intervall), ev Malaria
Schnelltest, Serologie hat keinen Stellenwert!
innerhalb 3 Wochen an virale Infekte denken!
Dengue, Chikungunya, VHF, …!
Typhus abdominalis, extraintestinale Amöben
Evison et al., 2005, PMID 15999931 // Nilles et al., 2012, PMID 21908138 /Maltha et al., 2013, PMID 23373854 // Wilson, 2012, PMID
22550113/
Fieber + Reiserückkehrer
nach Tropen: immer Malaria ausschliessen!!
Symptome unspezifisch: Fieber, Kopfschmerzen und
Malaise am häufigsten !
http://infekt.ch/unser-angebot/
Reiseort und Zeit? Malariarisiko? Wurde Prophylaxe
genommen? Moskito-Schutz? (Subsahara-Afrika höchstes Risiko)!
reisemedizin/
3x dicker Tropfen (febril, 12-24h Intervall), ev Malaria
Schnelltest, Serologie hat keinen Stellenwert!
innerhalb 3 Wochen an virale Infekte denken!
Dengue, Chikungunya, VHF, …!
Typhus abdominalis, extraintestinale Amöben
Evison et al., 2005, PMID 15999931 // Nilles et al., 2012, PMID 21908138 /Maltha et al., 2013, PMID 23373854 // Wilson, 2012, PMID
22550113/
Fieber und Infekte im Alter
Fieber als Kardinalsymptom ist im Alter oft
abgeschwächt oder in bis 30% nicht vorhanden!
Symptome sind oft schwächer, oft atypische
Präsentation (diagnostische Verzögerung!)!
Infektanfälligkeit und Outcome im Alter schlechter!
prinzipiell jede Änderung des funktionelles Status
kann Folge eines Infektes sein!
häufiges Symptom: Änderung der kognitiven
Fähigkeiten (auch wenn kein ZNS Infekt)!
Fieber bedeutet meist eine schwere Erkrankung
Norman, 2000, PMID 10913413 // Keating et al., 1984, PMID 6707408 // van Duin, 2012, PMID 22186775 // High et al., 2009, PMID 19072244
Fieber und Infekte im Alter
bei (1) jeder
‣An Infekt denken
Fieber als Kardinalsymptom
ist im Alter oft
abgeschwächt oder in bis 30% nicht vorhanden!
Änderung desSymptome
funktionellen
Status
sind oft schwächer, oft atypische
(diagnostische
Verzögerung!)!
(insbesonderePräsentation
kognitiv)
und
(2) Fieber!
Infektanfälligkeit und Outcome im Alter schlechter!
‣cave: Fieber in bis 30% abwesend!
prinzipiell jede Änderung des funktionelles Status
eines Infektes
sein!
einFolgeInfekt
wahrscheinlich
‣Bei Fieber istkann
häufiges Symptom: Änderung der kognitiven
Fähigkeiten (auch wenn kein ZNS Infekt)!
Fieber bedeutet meist eine schwere Erkrankung
Norman, 2000, PMID 10913413 // Keating et al., 1984, PMID 6707408 // van Duin, 2012, PMID 22186775 // High et al., 2009, PMID 19072244
Zusammenfassung der wichtigsten Leitsymptome
hohes Fieber >39°C
Erwachsene: Warnzeichen für eine schwere bakterielle Infektion DD:
Influenza, maligne Hyperthermie, malignes Neuroleptikasyndrom,
Medikamentenfieber
Hypothermie
Ältere Patienten: schwere, bakterielle Infektion, prognostisch schlechtes
Zeichen
Schüttelfrost
Zeichen einer Bakteriämie / bakteriellen (Endo-)Toxinen in der Blutbahn
Cave: Frösteln bei Fieberanstieg (auch bei viralen Infektionen und nicht
infektiösem Fieber)
rasch auftretende Petechien
Warnzeichen: Meningokokkeninfektion, akute Endokarditis, Sepsis,
hämorrhagisches Fieber. DIC, Vaskulitis, septische Emboli
Halsschmerzen und Stridor
DD: Epiglottitis, Peritonsillar-, Retropharyngeal- oder bei Halsschmerzen
Zungengrundabszess, (selten Diphtherie)
Meningismus
Kardinalsymptom der Meningitis. Kann bei älteren, komatösen und
intoxikierten Patienten fehlen oder nur diskret sein!
ZNS Symptome
Bewusstseinsstörung, Kopfschmerz, Krampfanfälle, fokale Ausfälle. DD:
Meningitis, Enzephalitis, Hirnabszess, Endokarditis
Immunsuppression
Breite DD (Viren, Bakterien, Pilze), inkl. opportunistische Erreger. Schwere
Immunsupression (Neutropenie, HIV Infektion): !
Risiko des fulminanten Verlaufs. Steroidtherapie kann die Fieberreaktion
unterdrücken oder verzögern
Alter
Atypische Klinik: Hypothermie bei schwerer Infektion, Meningitis ohne
Meningismus. Dehydratation, rascher Verlauf
Reiseanamnese
Spezielle Epidemiologie des Reiseziels beachten. Wichtige DD: Malaria,
Typhus, <21d auch: Dengue, HIV, VHF, etc
Asplenie (anat / funktionell)
Lebenslanges Risiko für fulminant verlaufende bakterielle Infektionen (vor
allem Pneumokokken)
Evison et al., 2005, PMID 15999931
Fragen und Diskussion
Infektiologische Notfälle in der Praxis