Erbliche Muskelerkrankungen - Ruhr
Werbung

Erbliche Muskelerkrankungen
‐ Morbus Duchenne / Becker ‐ Gliedergürtel‐Muskeldystrophien ‐ Maligne Hyperthermie Dystrophinopathien
Muskeldystrophie Duchenne
Muskeldystrophie Becker
Einschlusskörpermyopathie 2
Einschlusskörpermyopathie 3
Einschlusskörpermyopathie IBMPFD1
Einschlusskörpermyopathie IBMPFD2
Einschlusskörpermyopathie IBMPFD3
Envelopathien/Emery‐Dreyfuss‐Muskeldystrophien Emerinopathie; Laminopathie
Gliedergürteldystrophien
Gliedergürtel‐Muskeldystrophie‐Typ 1A
Gliedergürtel‐Muskeldystrophie‐Typ 1B
Gliedergürtel‐Muskeldystrophie‐Typ 1C
Gliedergürtel‐Muskeldystrophie‐Typ 1D
Gliedergürtel‐Muskeldystrophie‐Typ 1E
Gliedergürtel‐Muskeldystrophie‐Typ 1F
Gliedergürtel‐Muskeldystrophie‐Typ 1G
Gliedergürtel‐Muskeldystrophie‐Typ 1H
Gliedergürtel‐Muskeldystrophie‐Typ 2A
Gliedergürtel‐Muskeldystrophie‐Typ 2B
Gliedergürtel‐Muskeldystrophie‐Typ 2C
Gliedergürtel‐Muskeldystrophie‐Typ 2D
Gliedergürtel‐Muskeldystrophie‐Typ 2E
Gliedergürtel‐Muskeldystrophie‐Typ 2F
Gliedergürtel‐Muskeldystrophie‐Typ 2G
Gliedergürtel‐Muskeldystrophie‐Typ 2H
Gliedergürtel‐Muskeldystrophie‐Typ 2I
Gliedergürtel‐Muskeldystrophie‐Typ 2J
Gliedergürtel‐Muskeldystrophie‐Typ 2K
Gliedergürtel‐Muskeldystrophie‐Typ 2L
Gliedergürtel‐Muskeldystrophie‐Typ 2M
Gliedergürtel‐Muskeldystrophie‐Typ 2N
Gliedergürtel‐Muskeldystrophie‐Typ 2O
Gliedergürtel‐Muskeldystrophie‐Typ 2P
Gliedergürtel‐Muskeldystrophie‐Typ 2Q
Gliedergürtel‐Muskeldystrophie‐Typ 2R
Gliedergürtel‐Muskeldystrophie‐Typ 2S
Kardiomyopathien (>50 Formen) Dilatative Kardiomyopathie (MYBPC3)
Dilatative Kardiomyopathie (LMNA)
Dilatative Kardiomyopathie (SGCD)
Kongenitale Myasthenien Kongenitale Myasthenie (MUSK)
Kongenitale Myasthenie (RAPSN)
>6 weitere Formen Kongenitale Myopathien
Bethlem‐Myopathie
Fukuyama‐MDC
Muscle‐Eye‐Brain disease
Walker‐Warburg Syndrom
Walker‐Walker Syndrom Kongenitale Muskeldystrophie Typ 1B
Kongenitale Muskeldystrophie Typ 1C
Kongenitale Muskeldystrophie Typ 1D
Myotubuläre Myopathie
Nemaline Myopathie 1
Nemaline Myopathie 2
Nemaline Myopathie 3 Nemaline Myopathie 4 Nemaline Myopathie 5
Nemaline Myopathie 6
Nemaline Myopathie 7
Nemaline Myopathie 8
Ullrich‐Myopathie
Myofibrilläre Myopathien
Myofibrilläre Myopathie 1
Myofibrilläre Myopathie 2
Myofibrilläre Myopathie 3
Myofibrilläre Myopathie 4
Myofibrilläre Myopathie 5
Myofibrilläre Myopathie 6
Myotonien/Myot. Dystrophien Kongenitale Muskeldystrophie Typ 1A
Hypokaliämische periodische Paralyse 1
Hypokaliämische periodische Paralyse 2
Myotone Dystrophie 1
Myotone Dystrophie 2
Myotonia congenita Thomsen
Paramyotonia congenita
Proximale myotone Myopathie DM2/PROMM
Myotonia congenita Becker
Struktur‐Myopathien
Central‐Core‐Myopathie
Multiminicore‐Myopathie
Maligne Hyperthermie 1‐6
Rigid‐Spine‐Syndrom
Weitere Muskeldystrophien Fazioskapulohumerale Muskeldystrophie 1
Fazioskapulohumerale Muskeldystrophie 2
Okulopharyngeale Muskeldystrophie
Einschlusskörper‐Myopathien
ad
erbliche
Muskelleiden
Pseudo‐
hypertrophie
Lordosis,
scapulae alatae
Gower Manöver
DMD / BMD: klinische Aspekte
DMD
BMD
• 1:3500 neugeborene Jungen • spätes Laufen, im 3.‐5. LJ Symptome
• Lebenserwartung 20 Jahre
• progressive Skelettmuskel‐Dystrophie
• pseudohypertr. Waden, „Engelsflügel“
• Creatinkinase im Blut
• Herzmuskel affiziert, EKG!
• 1/3 mentale Retardierung
• glatte Muskulatur, Retina betroffen
• 1:35000 neugeborene Jungen
• mildere Symptome, bes. frühkindl.
• selten spätes Gehen lernen
• >20 J. Rennen, Treppensteigen
• im mittleren Lebensalter Gehen
• Creatinkinase im Blut
• oft Lernprobleme
• fertil
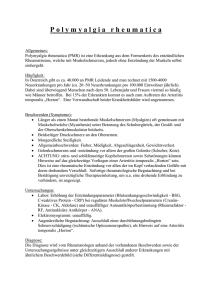
Dystrophin‐Protein
DMD / BMD: „Selbstheilung“ durch alternative mRNAs ?
alternative Dystrophin mRNAs:
1. alternative Promotoren
2. alternatives Spleißen
3. alternative Polyadenylierung
Dystrophin‐Promotoren + ‐Isoformen
gesamt
B, Gehirn M, Muskel P, Purkinje‐Zelle
R, Retina
B,K, Gehirn + Niere
S, Schwann‐Zelle
G, allgemein Dystrophin + interagierende Proteine
Dp260
Dp140
Exon
Protein‐
Homo‐
logie
Dystrophin
427 kD
ab1
Dp116
ab2
Actin‐
Bindung
rod Domänen
ß‐Dystroglycan/Syntrophin‐
Dp71
Bindung
ab3
ab2
ab1
Dystrophinopathie
Protein (427kD): 0.002 % der Muskelmasse
Therapie DMD: symptomatisch,
Genersatz‐Therapie
experimentelle Strategien:
‐ mini Dystrophin Gene / Hoch‐Kapazität Vektoren
‐ Utrophin Genexpression
‐ Stammzell‐Therapie
Dystrophinopathie
Stammzell‐Therapie
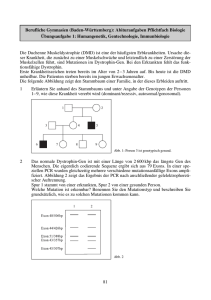
DMD / BMD: Genetik
• X chromosomal rezessiv
• Xp21; 2.3 Mb; 79 Exons
• 14 kb Transcripte; gewebsspezifische Isoformen
• 1/3 Punktmutationen
• 2/3 Deletionen/ Rearrangements/ Insertionen
• 1/3 Neumutationen
DMD / BMD: Deletionen
hotspot für Deletionen
Intron 44
Exon 44
• Deletionen sehr variabel
• DMD: meist Leserahmen ‐
• BMD: meist Leserahmen +
Dystrophin‐Mutationen
Mutationstyp
Anzahl Mutationen
Missense/nonsense
293
Spleißen 158
regulatorisch 0
kleine Deletion 165
kleine Insertion 52
kleine indel
12
grosse Deletion
1901
grosse Insertion 334
komplexes Rearrangement 24
Dystrophin‐Genvariationen http://www.dmd.nl/DMD_deldup.html
Variation
n =
position
5‘ UTR
Substitution
coding
intron
3‘UTR
20391
120
4067
16002
202
Deletion
2514
3
626
1670
215
Duplikation
2134
6
209
1560
359
466
2
26
434
4
56
41
Insertion
Insertion + Deletion
97
2 Variationen in 1 Allel
202
komplex + unbekannt
199
26005
2
131
4984
19709
780
DMD / BMD: Punktmutationen
• BMD: meist missense Mutationen im N‐/C‐Terminus oder Punktmutationen in Spleissstellen ohne Leserahmenstörung
• DMD: meist nonsense Mutationen (überall im Gen verteilt) oder Leserahmen‐
Störung durch Indel etc.
PTC124 (Ataluren) + AON
nonsense Mutationen Translationsstop
‐ Therapie: PTC124 read‐through
Stop‐Codon wird „fehl“‐translatiert ‐ Dystrophin‐Produktion in Zellkultur
‐ verbesserte Muskelfunktion im Mausmodell
‐ klinische Phase I‐ / II‐Studien
Exon‐skipping mit AON (antisense‐Oligonukleotid)
‐ klinische Studien fortgeschritten
kompen‐
satorische Proteine
kompensator.
Mechanismen
+ therapeut.
Strategien
Membran‐
Stabili‐
satoren Dystroglycan‐
Glykosylierung
kompensator. Proteine
Suppression des vorzeitigen Stopcodons (PTC 124) AS‐Ersatz normal Stopkodon Ersatz‐
Protein Spleißosom
normales Protein DMD‐Deletion, trunkiert
Exon übersprungen Spleißen
Exon A
U
1
U
2
Intron 1
Exon A
sf
sf
U
1
Exon B
Exon B
Intron 2
U
2
Exon C
+
Exon C
Intron 1
Intron 2
SSO – mediated splice switching
Exon A
U
1
Exon A
sf
Intron 1
SSO
Exon C
Exon B
Mutation
+
Intron 2
Intron 1
sf
Exon B
U
2
sf
Exon C
DMD / BMD Diagnose
DNA‐Sequenzanalyse
+ MLPA, in situ Hybridisierung Deletionen
Proteinanalyse
• Western blot
• Immunohistochemie
RNA‐Analyse
• RT‐PCR /arrays
• Protein Truncation Test (PTT) nonsense Mutationen
M. Duchenne/Becker ♀♀
1 : 50 000 000
unsymmetrische X‐Inaktivierung
45X
2 Mutationen
Konduktorin: Cardiomyopathie?
X‐Chromosomen Inaktivierung
Zygote
XpXm
XpXm
Xp
Xp
XpXm
Xm
Xm
Xm
Xm
frühe Teilungen
Xp
Xp
zufällige X‐
Inaktivierung
Inaktivierungsmuster wird vererbt an alle Tochterzellen
Mosaik
t(X;4)(p21;q31)
Chr. 4
der(4)
X‐Chr.
der(X)
Conclusiones DMD / BMD
Gendiagnostik komplex ‐ meist definitive Ergebnisse
Genanalysen kausale Pathogenese
besser verstanden +
neue therapeutische Optionen ?
Gliedergürtelmuskel‐Dystrophien
Gliedergürtelmuskel‐Dystrophien
• progressive Leiden der Skelettmuskeln • initiale Symptome bei Kind / Erwachsenen • initiale Pathologie im Schultergürtel • meist Creatinkinase im Blut
• Histologie: Dystrophie der Muskelfasern
LGMD ‐ Differentialdiagnose
• alle Muskelleiden mit proximaler Komponente
–
–
–
–
–
–
neurogene Muskelatrophie
metabolische + mitochondriale Myopathien
inflammatorische Myopathien
myasthenische Syndrome
congenitale Strukturmyopathien
andere
LGMD ‐ Differentialdiagnose
‐Sarkoglykanopathie
Autosomal dominante LGMD
Form
Chromos.
Protein
LGMD1A 5q31
Myotilin
LGMD1B, ADEDMD...
1q21
Lamin A/C
LGMD1C
3p25
Caveolin 3
LGMD1E 7q
DNAJB6
LGMD1F
7q32
Transportin 3
LDMD1G
4q21
?
LGMD1H
3p23
? {aktualisiert 6.11.2014}
Form Chromosom
Protein
LGMD2A 15q
Calpain 3
LGMD2B
2p
Dysferlin
LGMD2C‐2F
13q, 17q, 4q, 5q
Sarkoglykans LGMD2G
17q
TCAP
LGMD2H
9q
TRIM32
LGMD2I
19q
Fukutin‐rel. protein
LGMD2J
2q
Titin
LGMD2K
9q
POMT‐1
LGMD2L
11p
ANO5
LGMD2M
9q
FKTN
LGMD2N
14q
POMT2
LGMD2O
1p
POMGNT1
LGMD2P
3p
DAG1
LGMD2Q
8q
Plectin
LGMD2R
2q
DES
LGMD2S
4q
TRAPPC11
{aktualisiert 6.11.2014}
6 J.:
9 J.: • auffälliges Gangbild • Zehengang
• Stolpern & Fallneigung
• Muskelschwäche Schulter‐ + Beckengürtel
• Kniebeugen unmöglich, Treppensteigen
A.D.
Labor: Creatinkinase GOT GPT LDH 6360 U/l
138 U/l
156 U/l
1070 U/l
Myosonographie & Elektromyogramm: Myopathie
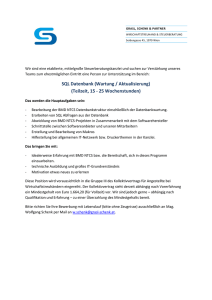
Biopsie m. vastus lateralis:
HE Immunohistologie Western blot Diagnose: dystrophischer Muskel
Muskelfaser schwach pos. für Dys‐1, negativ für Dys‐2 Dystrophin <5%
Morbus Duchenne
Molekulargenetik: Deletion im Dystrophin‐Gen
bis 12 J.:
Symptome; 12 J. Gehen,
Muskelkraft
17 J.: Stehen
Kontrakturen Hüfte, Knie‐, Armgelenke
Lungenfunktion o.B., CK 617 U/l
atypischer M. Duchenne‐Verlauf Diagnose‐Reevaluation
Rebiopsie: • aktiver dystrophischer Prozess
• einzelne Fasern negat. für Dys 2‐Antikörper
• Dys 1‐ + 3‐Antikörper o.B.
• a‐Sarkoglykanprotein
• b‐, g‐, d‐Sarkoglykan o.B.
Arg77Cys
Tyr134TER
Erbliche Muskelerkrankungen
‐ Morbus Duchenne / Becker ‐ Gliedergürtel‐Muskeldystrophien ‐ Maligne Hyperthermie Maligne Hyperthermie
Maligne Hyperthermie
MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS1 (RYR1)
MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS2 MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS3 MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS4 MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS5 (CACNA1S)
MALIGNANT HYPERTHERMIA, SUSCEPTIBILITY TO, MHS6 19q13.1
17q11.2‐q24
7q21‐q22
3q13.1
1q32
5p
NATIVE AMERICAN MYOPATHY 4
CONTRACTURES, CONGENIT., TORTICOLLIS, MALIGNANT HYPERTHERMIA 7
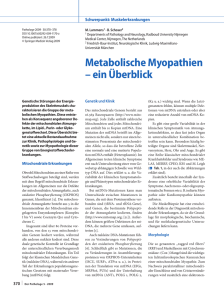
RYR1 Gen + Protein
Calzium
Homer
Triadin
FKBP12
S1000A1
DHPR
Calmodulin
LIZ Motive (Phosphorylierung)
SPRY Domänen)
Mutations hotspots
Protein
N‐Terminus
C‐Terminus
Rigor
°C
CO2
Laktat
RYR1 – Proteinmodell
Tiermodelle für MH
Central Core Disease (CCD)
• congenitale Myopathie
• RYR‐Mutationen
• Mutationsanalyse: 41 Exons
• Vererbung
‐ autosomal dominant
‐ selten autosomal rezessiv
Interaktion zwischen Dihydropterin‐Reduktase (DHPR) und RYR1 zur Ca2+‐Freisetzung Membran‐
Depolarisation
terminale Zysterne
T‐Tubulus
Central core disease
90% Mutationen im RYR1 Gen…
…in den gleichen Bereichen wie bei MH
Erbliche Muskelerkrankungen
werden zunehmend besser verstanden,
aber wann kommt kausale Therapie ?