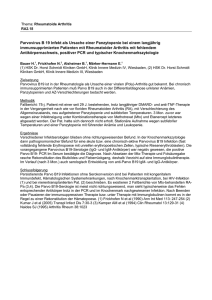
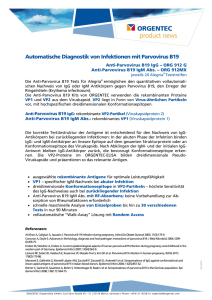
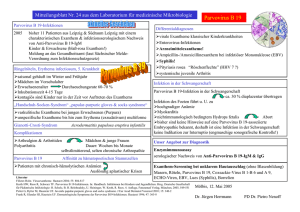
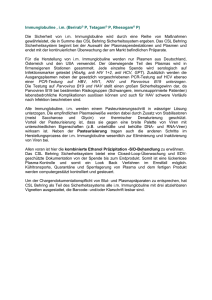
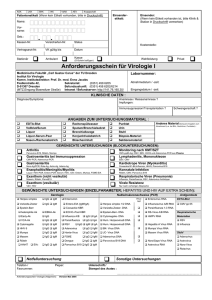
RIDA Blot Parvovirus B19
Werbung

RIDA® Blot Parvovirus B19 Immunoblot mit rekombinanten Antigenen zum Nachweis von Antikörpern (IgM/IgG) gegen das humane Parvovirus B19 Immunoblot with recombinant antigens for the detection of antibodies (IgM/IgG) against the human parvovirus B19 Art. No.: L 6003 Y In vitro Test Lagerung bei 2 - 8 °C Storage at 2 - 8 °C R-Biopharm AG, Darmstadt, Germany Tel.: +49 (0) 61 51 81 02-0 / Telefax: +49 (0) 61 51 81 02-20 Anschrift: R-Biopharm AG Landwehrstr. 54 D-64293 Darmstadt Für weitere Fragen stehen Ihnen gerne zur Verfügung: Telefon: Zentrale / Auftragsannahme Sekretariat Marketing (0 61 51) 81 02-0 (0 61 51) 81 02-23 Telefax / E-Mail: Auftragsannahme (0 61 51) 81 02-20 [email protected] Marketing (0 61 51) 81 02-40 [email protected] RIDA® und RIDASCREEN® sind eingetragene Warenzeichen der R-Biopharm AG Hersteller: R-Biopharm AG, Darmstadt, Deutschland RIDA® and RIDASCREEN® are registered trademarks of R-Biopharm AG Manufacturer: R-Biopharm AG, Darmstadt, Germany 2 RIDA® Blot Parvovirus B19 03-11-11 Inhaltsverzeichnis Seite 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Allgemeines .................................................................................................... 4 Einleitung ........................................................................................................ 4 Testprinzip ...................................................................................................... 6 Packungsinhalt ............................................................................................... 6 Zusätzlich benötigte Reagenzien - erforderliches Zubehör ............................ 7 Vorsichtsmaßnahmen ..................................................................................... 7 Reagenzien und ihre Lagerung ...................................................................... 8 Anzeichen für Reagenzienverfall .................................................................... 8 Sammlung und Lagerung der Proben............................................................. 8 Testdurchführung............................................................................................ 8 Auswertung.................................................................................................... 12 Hinweise zur Testdurchführung und Interpretation ........................................ 15 Klinische Ergebnisse ..................................................................................... 18 Contents page 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Intended use .................................................................................................. General .......................................................................................................... Test principle ................................................................................................. Reagents provided......................................................................................... Materials required but not provided ............................................................... Warnings and precautions for the users ........................................................ Storage instructions ....................................................................................... Indication of instability or deterioration of reagents........................................ Specimen collection and storage ................................................................... Test procedure............................................................................................... Analysis ......................................................................................................... Remarks about the test procedure and interpretation.................................... Clinical results................................................................................................ 20 20 22 22 23 23 24 24 24 24 28 30 34 Appendix Literature ............................................................................................................. 35 RIDA® Blot Parvovirus B19 03-11-11 3 1. Allgemeines Für die in vitro Diagnostik. Der RIDA® Blot Parvovirus B19 ist ein qualitativer Test zum Nachweis und zur Identifizierung von Antikörpern (IgM und IgG) gegen das Parvovirus B19 in humanem Serum oder Plasma. Der Test erlaubt durch die elektrophoretische Auftrennung rekombinant hergestellter Bestandteile des Virusproteins im Unterschied zu anderen Testverfahren eine Aussage über das Vorhandensein unterschiedlicher Antikörper, die wiederum verschiedenen Krankheitsstadien zugeordnet werden können. 2. Einleitung Das humane Parvovirus B19 wurde 1975 von Cossart und Mitarbeitern in England entdeckt. Sie fanden dieses Virus beim Screening von Blutspenderseren auf Hepatitis B. Sie bezeichneten dieses zufällig gefundene Isolat mit B19. Das Parvovirus B19 ist ein kleines, nicht umhülltes DNA-Virus mit einem Durchmesser von 18 - 26 nm. Das Genom besteht aus Einzelstrang-DNA von 5,4 Kilobasen Länge. Das Kapsid besteht aus 2 Polypeptiden der Größen 84 kD und 58 kD (VP1 und VP2). Beide Strukturproteine sind in einem gemeinsamen Leserahmen auf dem viralen Genom kodiert, wobei das kürzere VP2 einen späteren Transkriptionsstart im Leserahmen von VP1 besitzt (siehe Pkt. 12). Das bedeutet, daß beide Proteine bis auf einen zusätzlichen N-terminalen, etwa 26 kD großen Teil von VP1 identisch sind. Weiterhin ist im Genom noch ein Haupt-Nicht-Strukturprotein (NS-1) kodiert, welches für die Virusreplikation und Vermehrung nötig ist. Das B19-Virus ist von ikosaedrischer Struktur und sehr hitzestabil. Es kann eine Temperatur von 60°C bis zu 12 Stunden lang überstehen. Zur Gattung der Parvoviren gehören neben dem einzigen, bisher bekannten humanpathogenem Parvovirus B19 auch eine Reihe tierpathogener Viren wie das Hundeparvovirus und das Katzen-Panleukopenievirus. Die Parvoviren bilden zusammen mit den Densoviren und den Dependoviren, deren Vermehrung ein Hilfsvirus (Adeno- oder Herpesviren) benötigt, die Familie der Parvoviridae. Eine hervorzuhebende Eigenschaft der Parvoviren ist die selektive Replikation in sich teilenden Zellen wie Knochenmark-, Darm- und Embryonalzellen. Infektionen mit dem weltweit verbreiteten humanen Parvovirus B19 treten saisonal gehäuft im Winter und Frühsommer auf und können vor allem in Kindergärten und Schulen zu Epidemien führen. Die Übertragung erfolgt hauptsächlich über den Respirationstrakt (Tröpfcheninfektion), kann aber auch über Blut und Blutprodukte erfolgen. Frische Parvovirus-Infektionen treten in allen Altersstufen auf, am häufigsten in der Altersgruppe zwischen 6 und 15 Jahren. Die Durchseuchungsrate steigt mit dem Lebensalter und erreicht im Erwachsenenalter einen Wert von etwa 40 - 70%. Frauen zeigen dabei eine höhere Prävalenz als Männer. 4 RIDA® Blot Parvovirus B19 03-11-11 Die Inkubationszeit beträgt 1 - 3 Wochen, wobei sich die virämische Phase, in der der Patient als infektiös gilt, auf 3 - 7 Tage beschränkt. In dieser Zeit kann der Patient asymptomatisch sein oder über eine geringe Allgemeinsymptomatik wie Kopfschmerzen, Juckreiz, Myalgien und Fieber klagen. Etwa ab der zweiten Woche nach der Infektion kann das Erythema infectiosum (Ringelröteln) auftreten. Während bei Kindern überwiegend typische Exantheme auftreten (Wangenrötung, girlandenförmige febrile Purpura insbesondere an den Streckseiten der Extremitäten), sind sie bei Erwachsenen eher untypisch. Zur weiteren Symptomatik einer B19-Infektion gehören Arthralgien und Arthritiden (60%), respiratorische Symptome (22%) sowie Durchfälle (15 - 35%). Nur etwa 20% aller Parvovirus B19Infektionen verlaufen symptomlos. Frauen sind dabei von Gelenkbeschwerden doppelt so häufig betroffen wie Männer. Diese Arthropathien verschwinden in den meisten Fällen innerhalb von zwei bis vier Wochen. In wenigen Fällen können die Symptome aber jahrelang intermittierend fortbestehen, so daß bei der Abklärung chronischer Arthropathien auch an eine persistierende Parvovirus B19-Infektion gedacht werden muß. Während die durch Parvovirus B19 bedingte Hemmung der Erythropoese (Dauer 1 - 4 Wochen) beim gesunden Menschen meist subklinisch bleibt, gipfelt sie bei Patienten mit chronisch hämolytischen Anämien (Sichelzellenanämie, Thalassämie, Pyruvatkinasemangel, Sphärozytose, autoimmun-hämolytische Anämie) häufig in einer aplastischen Krise. Solche Patienten sind transfusionsbedürftig und sollten in ein Krankenhaus eingewiesen werden. Zusätzliche Organmanifestationen wie etwa hepatische Dysfunktionen oder eine B19-assoziierte Myokarditis sind in jüngster Zeit beschrieben worden. Zu einer weiteren Komplikation nach einer B19-Infektion kann es bei seronegativen Schwangeren kommen. Das Parvovirus B19 kann transplazentar auf den Föten übertragen werden. Aufgrund der kurzen Lebensdauer der Erythrozyten bis zur 20. Schwangerschaftswoche und einer fehlenden effizienten Immunabwehr kann eine Infektion zu einer schweren akuten oder chronischen Anämie mit nachfolgendem Spontanabort führen. Eine weitere Komplikation nach Infektion während des zweiten Trimenons ist die Ausbildung eines Hydrops fetalis. Über 80% der Schwangerschaften verlaufen jedoch komplikationslos. Embryopathien sind bislang nicht beobachtet worden. Antikörper der Klasse IgM können etwa 10 Tage nach Infektion und damit meist gleichzeitig mit dem Beginn der Symptome nachgewiesen werden, IgG-Antikörper sind bereits wenige Tage später zu finden und persistieren in der Regel lebenslang. IgM-Antikörper sind hingegen meist nach 30 bis 60 Tagen nicht mehr nachweisbar. Zum Nachweis von Antikörpern eignen sich Elisasysteme auf der Basis rekombinanter VP1/VP2-Peptide. Wegen der besseren Aussagekraft über das mögliche Stadium der Erkrankung durch den Nachweis unterschiedlicher Antikörper sollte immer ein Western Blot, wie der RIDA® Blot Parvovirus B19, der verRIDA® Blot Parvovirus B19 03-11-11 5 schiedene rekombinant hergestellte Bestandteile des Virusantigens verwendet, angeschlossen werden. 3. Testprinzip Für den vorliegenden Immunoblot werden vier rekombinante Parvovirus B19-Antigene verwendet, die in E. coli erzeugt werden. Es handelt sich dabei um Teile der beiden Strukturproteine VP1 und VP2 und um das Haupt-Nicht-Strukturprotein NS-1 (siehe Pkt. 12.). Die gereinigten (frei von Fusionsproteinen), rekombinanten Antigene wurden elektrophoretisch nach ihrem Molekulargewicht aufgetrennt und anschließend auf eine Nitrocellulose-Membran geblottet. Die Membran wurde danach in einzelne Blotstreifen zerschnitten. Diese Streifen werden mit der zu untersuchenden Probe (Serum, Plasma) inkubiert, wobei die darin vorhandenen Antikörper an die spezifischen Proteinbanden binden. Nach Beseitigung ungebundener Antikörper durch Waschen der Streifen werden in einer zweiten Inkubation mit anti-human IgModer IgG-Konjugat (Peroxidase) und anschließender Farbreaktion spezifisch gebundene Antikörper gegen die vier Antigene des Parvovirus B19 als blaue Banden auf den Streifen sichtbar. 4. Packungsinhalt Die Reagenzien einer Packung reichen für 20 Bestimmungen. Jeder Reagenziensatz enthält: 2 x 10 Teststreifen; beschichtet mit rekombinanten Parvovirus B19-Antigenen 1 x Wasch- / Verdünnungspuffer (100 ml, 5fach konz.); enthält Tris-Puffer, NaCl, Tween-20 und Protein 1 x schwach positive IgM Kontrolle (80 µl); rote Verschlußkappe Humanserum, enthält < 0,1% NaN3 1 x schwach positive IgG Kontrolle (80 µl); weiße Verschlußkappe Humanserum, enthält < 0,1% NaN3 1 x Negativkontrolle (80 µl); blaue Verschlußkappe Humanserum, enthält < 0,1% NaN3 1 x Anti-human IgM-Konjugat (100 µl, 500fach konz.); lila Verschlußkappe Kaninchen, Meerrettich-Peroxidase konjugiert, enthält < 0,1% NaN3 1 x Anti-human IgG-Konjugat (60 µl, 1000fach konz.); grüne Verschlußkappe Kaninchen, Meerrettich-Peroxidase konjugiert, enthält < 0,1% NaN3 6 RIDA® Blot Parvovirus B19 03-11-11 1 x Substrat (45 ml); gebrauchsfertig, enthält Tetramethylbenzidin (TMB) 2 x Inkubationswannen à 10 Vertiefungen 1 x Kontrollstreifen (entwickelt, kitspezifisch) 1 x Gebrauchsanleitung 2 x Protokollblätter 5. Zusätzlich benötigte Reagenzien - erforderliches Zubehör 5.1. Reagenzien − Deionisiertes Wasser 5.2. Zubehör − Vakuumpumpe zum Absaugen der Flüssigkeit aus den Inkubationswannen − Pipetten für 2 - 10 µl, 10 - 100 µl und 2 ml − Meßzylinder für 100 ml und 500 ml − Schüttler − Plastikpinzette zum Anfassen der Nitrozellulose-Streifen 6. Vorsichtsmaßnahmen Nur für die in vitro Diagnostik. Dieser Test ist nur von geschultem Laborpersonal durchzuführen. Die Richtlinien zur Arbeit in medizinischen Laboratorien sind zu beachten. Die Gebrauchsanweisung zur Durchführung des Tests ist strikt einzuhalten. Proben oder Reagenzien nicht mit dem Mund pipettieren, Kontakt mit verletzter Haut oder Schleimhäuten vermeiden. Während des Umgangs mit Proben EinmalHandschuhe tragen und nach Abschluss des Tests die Hände waschen. In den Bereichen, in denen mit den Proben oder den Test-Reagenzien gearbeitet wird, nicht rauchen, essen oder trinken. Die im Kit befindlichen Kontrollseren (Positiv- und Negativkontrolle) wurden auf HIV 1+2- und HCV-Ak sowie HBsAg untersucht und für negativ befunden. Dennoch sollten sie, ebenso wie die Patientenproben und alle Materialien, die mit ihnen in Berührung kommen, als potentiell infektiös behandelt und entsprechend den jeweiligen nationalen Sicherheitsbestimmungen gehandhabt werden. Die Konjugate und die Kontrollen enthalten Natriumazid. Eine Berührung mit der Haut oder Schleimhaut ist zu vermeiden. Bei Kontakt mit Blei- oder Kupferrohren können explosive Metallazide entstehen. RIDA® Blot Parvovirus B19 03-11-11 7 Sämtliche Reagenzien und Materialien, die mit potentiell infektiösen Proben zusammenkommen, müssen mit geeigneten Desinfektionsmitteln behandelt oder mindestens eine Stunde bei 121 °C autoklaviert werden. 7. Reagenzien und ihre Lagerung Alle Reagenzien sind bei 2 – 8 °C zu lagern und bis zu dem auf den Etiketten aufgedruckten Verfalldatum verwendungsfähig. Reagenzien aus Kits verschiedener Chargen dürfen nicht miteinander kombiniert werden. Mikrobielle Kontamination ist zu vermeiden. Die konzentrierten Konjugate und Puffer sind jeweils frisch zu verdünnen. 8. Anzeichen für Reagenzienverfall Eine fehlende Reaktion der Inkubationskontrolle oder ein Fehlen von Banden bei den Positivkontrollen, so dass diese die unter Punkt 11. genannten Forderungen nicht mehr erfüllen, können Hinweise für einen Reagenzienverfall sein. Die Packungen tragen ein Verfallsdatum, nach dessen Erreichen keine Qualitätsgarantie mehr übernommen werden kann. 9. Sammlung und Lagerung der Proben Der RIDA® Blot Parvovirus B19 kann mit Serum oder Plasma durchgeführt werden. Hitzeinaktivierte Proben können zu erhöhten Hintergrundreaktionen führen. Wiederholtes Einfrieren und Auftauen der Proben ist unbedingt zu vermeiden, ebenso mikrobielle Kontamination. Die Verwendung von lipämischen, hämolytischen oder trüben Proben kann eine dunkle Hintergrundfärbung der Streifen hervorrufen. Diese Proben können darüber hinaus zu verfälschten Ergebnissen führen und sollten daher nicht verwendet werden. Sollte die Bestimmung nicht sofort erfolgen, kann das Probenmaterial bis zu zwei Wochen bei 2 – 8 °C aufbewahrt werden. Eine längere Lagerung der Proben ist durch Aufbewahrung bei –20 °C oder tiefer möglich. 10. Testdurchführung 10.1. Allgemeines Vor Testbeginn müssen alle Kitkomponenten für mindestens 30 Minuten auf Raumtemperatur gebracht werden. Das Röhrchen mit den Teststreifen ist erst anschließend zu öffnen, um eine Kondenswasserbildung zu vermeiden. Die nicht benötigten Streifen verbleiben im Röhrchen und werden weiterhin bei 2 - 8°C ge8 RIDA® Blot Parvovirus B19 03-11-11 lagert (Röhrchen wieder gut verschließen, Teststreifen dürfen vor Versuchsbeginn nicht feucht werden!). Es sollte nur soviel Reagenz entnommen werden, wie für die Durchführung des Tests benötigt wird. Überschüssiges Reagenz darf nicht in die Gefäße zurückgegeben werden, da dies zu einer Kontamination führen kann. Reagenzien und Streifen dürfen nicht verwendet werden, wenn die Verpackung beschädigt ist oder die Gefäße undicht sind. Die Streifen müssen nicht in der Reihenfolge ihrer Nummerierung eingesetzt werden. Es ist aber genau darüber Protokoll zu führen, welcher Streifen mit welcher Probe inkubiert wird. Die Reproduzierbarkeit von Western Blot Ergebnissen hängt in starkem Maße vom gleichmäßigen Waschen der Streifen ab. Die unten beschriebenen Waschsequenzen sollten deshalb immer eingehalten werden. Achtung! Die kleinen Reagenzgefäße sollten vor dem Öffnen ganz kurz zentrifugiert werden, damit sich die Flüssigkeit auf dem Boden des Gefäßes sammelt und keine Verluste entstehen. 10.2. Herstellung des gebrauchsfertigen Wasch- / Verdünnungspuffers Das Puffer-Konzentrat enthält eine lösliche Proteinkomponente. Das Konzentrat sollte vor dem Verdünnen kurz geschüttelt werden, um eine gleichmäßige Verteilung zu gewährleisten. Der verdünnte Puffer wird zum Waschen, für die Probenverdünnung und die Herstellung der Konjugatlösungen benötigt. Der Wasch- / Verdünnungspuffer ist stets frisch anzusetzen. Das benötigte Volumen ist für die Anzahl durchzuführender Tests zu bestimmen. Der verdünnte Wasch- / Verdünnungspuffer ist nicht haltbar. Nicht benötigter Puffer muß verworfen werden. Ein Teil des Pufferkonzentrats wird mit vier Teilen deionisiertem Wasser verdünnt (Verdünnung 1:5). Tabelle 1: Wasch- / Verdünnungspuffer pro eingesetzte Streifen eingesetzte Streifen Wasch- / Verdünnungspuffer-Konzentrat deionisiertes Wasser gebrauchsfertiger Puffer 2 5 10 15 20 10 ml 25 ml 50 ml 75 ml 100 ml 40 ml 100 ml 200 ml 300 ml 400 ml 50 ml 125 ml 250 ml 375 ml 500 ml RIDA® Blot Parvovirus B19 03-11-11 9 10.3. Erste Inkubation Eine der Bestimmungszahl entsprechende Anzahl Vertiefungen der Inkubationswannen wird mit je 2 ml des gebrauchsfertigen Wasch- / Verdünnungspuffers gefüllt. Pro Bestimmung wird ein Blotstreifen mit einer Pinzette dem Röhrchen entnommen (Streifen dabei nur am Ende mit der Nummerierung anfassen) und in den Puffer eingetaucht. Der Streifen muß vollkommen mit Puffer benetzt sein. Die Streifennummerierung muss nach oben zeigen. 20 µl der unverdünnten Probe (Serum oder Plasma) oder der jeweiligen schwach positiven Kontrolle bzw. der Negativkontrolle werden in die entsprechenden Vertiefungen gegeben. Die schwach positiven Kontrollen müssen entsprechend der Untersuchung (IgM oder IgG) bei jedem Versuchsansatz unabhängig von der Zahl der zu testenden Seren mit geführt werden. Es ist darauf zu achten, daß es zu keiner Kontamination benachbarter Vertiefungen und damit zu möglicherweise falsch positiven Resultaten kommt. Während der Inkubation sollten die Wannen mit den beigefügten Deckeln abgedeckt werden. Die Blotstreifen werden mit der Probe unter leichtem Schütteln über Nacht (10 bis 16 Stunden) bei Raumtemperatur (18 – 25 °C) inkubiert. 10.4. Waschen Die Inkubationslösung wird aus den Vertiefungen abgesaugt, vorzugsweise mit einer Absaugpumpe mit angeschlossener Desinfektionsfalle. Jeder Streifen wird dann viermal 5 Minuten mit je 2 ml gebrauchsfertigem Wasch- / Verdünnungspuffer unter leichtem Schütteln gewaschen. Zwischen den einzelnen Waschschritten wird der Puffer aus den Vertiefungen abgesaugt. Achtung! Während des letzten Waschschrittes ist die Konjugatlösung herzustellen. 10.5. Herstellung der Konjugatlösung Das Konjugat liegt im Kit in konzentrierter Form vor. Für die Verwendung im Test ist hiervon eine Verdünnung mit dem gebrauchsfertigen Wasch- / Verdünnungspuffer herzustellen. Da das verdünnte Konjugat nur eine begrenzte Stabilität aufweist ist es jeweils unmittelbar vor der Verwendung frisch anzusetzen. 10.5.1. IgM-Konjugat Für die Bestimmung von IgM-Antikörpern ist von dem im Kit befindlichen Antihuman IgM-Konjugat eine 1:501 Verdünnung herzustellen. Die hierfür benötigten 10 RIDA® Blot Parvovirus B19 03-11-11 Volumina für die entsprechende Anzahl von Streifen sind der Tabelle 2 zu entnehmen. Tabelle 2: Herstellung der gebrauchsfertigen IgM-Konjugatlösung eingesetzte Streifen Konjugat-Konzentrat gebrauchsfertiger Wasch- / Verdünnungspuffer 2 4 8 16 20 10 µl 20 µl 40 µl 80 µl 100 µl 5 ml 10 ml 20 ml 40 ml 50 ml 10.5.2. IgG-Konjugat Für die Bestimmung von IgG-Antikörpern ist von dem im Kit befindlichen Antihuman IgG-Konjugat eine 1:1001 Verdünnung herzustellen. Die hierfür benötigten Volumina für die entsprechende Anzahl von Streifen sind der Tabelle 3 zu entnehmen. Tabelle 3: Herstellung der gebrauchsfertigen IgG-Konjugatlösung eingesetzte Streifen Konjugat-Konzentrat gebrauchsfertiger Wasch- / Verdünnungspuffer 2 4 8 16 20 5 µl 10 µl 20 µl 40 µl 50 µl 5 ml 10 ml 20 ml 40 ml 50 ml 10.6. Zweite Inkubation Zu jedem Streifen werden 2 ml der entsprechenden gebrauchsfertigen Konjugatlösung pipettiert. Danach werden die Streifen eine Stunde unter leichtem Schütteln bei Raumtemperatur inkubiert. 10.7. Waschen Waschsequenz gemäß Pkt. 10.4. RIDA® Blot Parvovirus B19 03-11-11 11 10.8. Dritte Inkubation Zu jedem Streifen werden 2 ml des gebrauchsfertigen Substrats pipettiert. Die Streifen werden 5 - 15 Minuten bei Raumtemperatur inkubiert, bis die Intensität auf den Streifen, die mit den schwach positiven Kontrollen inkubiert wurden, den unter Punkt 11. genannten Forderungen entspricht. Danach wird das Substrat abgesaugt. Zum Stoppen der Färbereaktion werden die Streifen in den Wannen dreimal mit deionisiertem Wasser abgespült. Die Streifen werden vorsichtig mit einer Pinzette den Wannen entnommen und zum Trocknen zwischen saugfähiges Papier gelegt. Nach dem Trocknen können die Streifen ausgewertet werden. Achtung! Bei hoch positiven Seren kann es zu einer Überreaktion der Färbung kommen. Es wird empfohlen, bei solchen Streifen die Färbung vorzeitig zu beenden. Zusammenfassung der Testdurchführung 1. Alle Reagenzien werden auf Raumtemperatur gebracht 2. In jede Vertiefung werden 2 ml Verdünnungspuffer pipettiert 3. Pro Vertiefung wird ein Streifen in den Puffer gelegt 4. Zugabe von 20 µl Probe, schwach positiver oder Negativkontrolle 5. Inkubation bei Raumtemperatur über Nacht (10 - 16 h) 6. 4maliges Waschen mit 2 ml Waschpuffer; Verweildauer je 5 Min. 7. Zugabe von 2 ml frisch hergestellter Konjugatlösung 8. 1 Stunde Inkubation bei Raumtemperatur 9. 4maliges Waschen mit 2 ml Waschpuffer; Verweildauer je 5 Min. 10. Zugabe von 2 ml Substrat 11. 5 - 15 Minuten Inkubation bei Raumtemperatur 12. Spülen der Streifen mit deionisiertem Wasser 13. Trocknen auf Filterpapier 14. Auswertung 11. Auswertung Zur Überprüfung der Funktion des Testkits dienen die schwach positiven Kontrollen, die bei jeder Testdurchführung mitgeführt werden müssen, die Negativkontrolle sowie die Inkubations-Kontrollbande, die auf jedem Streifen vorhanden ist. 12 RIDA® Blot Parvovirus B19 03-11-11 Die Inkubations-Kontrollbande befindet sich unterhalb der Numerierung; sie besteht aus Protein A, das Globuline bindet, und muß deshalb bei korrekter Durchführung auf jedem Streifen sichtbar werden. Bei korrekter Durchführung sollte bei der schwach positiven IgG Kontrolle die Bande VP-N schwach, aber deutlich sichtbar sein; die Bande VP-C erscheint viel schwächer und relativ breit und diffus. Die Bande VP-1S reagiert mit diesem Serum nur sehr schwach oder gar nicht. Bei der schwach positiven IgM Kontrolle ist die Bande VP-N relativ deutlich sichtbar und die Bande VP-C nur sehr schwach. Bei der Negativkontrolle sollte neben der Inkubations-Kontrollbande keine weiter Bande sichtbar sein. Sollten die vorgegebenen Bedingungen nicht erfüllt sein, ist vor einer Testwiederholung folgendes zu überprüfen: − Haltbarkeit der verwendeten Reagenzien − Funktionsfähigkeit der eingesetzten Geräte (z. B. Kalibrierung) − Korrekte Testdurchführung − Visuelle Kontrolle der Kitkomponenten auf Kontamination oder Undichtigkeit Sind nach Testwiederholung die Bedingungen wiederum nicht erfüllt, wenden Sie sich bitte an den Hersteller. Zur besseren Dokumentation können die Streifen auf den beigelegten Protokollblättern aufgeklebt und die identifizierten Banden notiert werden. Die Protokollblätter sind mit Datum und Chargen-Nummer zu versehen. Zur Auswertung der Patientenprobe wird die Inkubations-Kontrollbande der Teststreifen mit der Kontrollbande des Streifens auf der Auswerteschablone in Übereinstimmung gebracht. Anhand der auf der Auswerteschablone vorhandenen Bandenbezeichnungen können dann die bei den Patientenproben sichtbaren Banden identifiziert werden. Die Intensität der identifizierten Banden wird mit der Intensität der Banden auf den Streifen mit der jeweiligen schwach positiven Kontrolle (IgM oder IgG) verglichen. Aufgrund dieses Vergleiches wird analog zur nachfolgenden Tabelle die Intensität der einzelnen Banden ermittelt und auf dem Protokollblatt notiert. RIDA® Blot Parvovirus B19 03-11-11 13 Tabelle 4: Auswertung der Bandenintensität Bandenintensität Bewertung - nicht sichtbar +/- sehr schwache Intensität + schwache Intensität (ähnlich der schwach positiven Kontrolle) gut sichtbare Intensität ++ starke Intensität +++ 11.1. Auswertung IgM-Nachweis Für die Positiv-/Negativ-Bewertung im Falle des IgM-Nachweises wird eine eventuell vorhandene Reaktivität von Antikörpern gegen das NS-1-Protein nicht berücksichtigt. Tabelle 5: IgM-Auswertung IgM positiv und VP-N mind. + VP-C mind. +/- andere Banden können, müssen aber nicht erscheinen IgM fraglich IgM negativ VP-N mind. + oder VP-C mind. + oder VP-N u. VP-C +/- keine Reaktion oder andere Konstellationen andere Banden können, müssen aber nicht erscheinen 11.2. Auswertung IgG-Nachweis Für die Positiv-/Negativ-Bewertung im Falle des IgG-Nachweises wird eine vorhandene Reaktivität von Antikörpern gegen das NS-1-Protein nicht berücksichtigt. Tabelle 6: IgG-Auswertung IgG positiv VP-N mind. + andere Banden können, müssen aber nicht erscheinen 14 IgG fraglich IgG negativ VP-C mind. + oder VP-N u. VP-C +/andere Banden können, müssen aber nicht erscheinen keine Reaktion oder andere Konstellationen, besonders schwache, isolierte Reaktion gegen VP-1S RIDA® Blot Parvovirus B19 03-11-11 11.3. Auswertung der Reaktivität gegen NS-1 Da Antikörper gegen dieses Protein nach heutigem Wissensstand nur bei persistierenden Parvovirus B19-Infektionen auftreten, wird eine Reaktivität gegen das NS-1 nicht für eine positive Bewertung des Western Blots herangezogen. Bisher wurden nur IgG-Antikörper gegen das NS-1 identifiziert, die frühestens sechs bis acht Wochen nach einer Infektion gefunden werden. Ein vorhandene Reaktivität gegen das NS-1 kann somit als ein Hinweis auf eine möglicherweise persistierende Infektion bewertet werden. 12. Hinweise zur Testdurchführung und Interpretation 12.1. Diagnostische Bedeutung rekombinanter B19 Antigene Das Parvovirus B19 Genom mit einer Größe von ca. 5,4 kb enthält die genetische Information für zwei Strukturproteine und ein Nicht-Strukturprotein (siehe Abb. 1). Aus den beiden Strukturproteinen VP1 und VP2 wird das Kapsid gebildet, das die DNA umgibt. Die beiden Strukturproteine mit Größen von 84 kD und 58 kD sind in einem gemeinsamen Leserahmen auf dem viralen Genom kodiert, wobei das kleinere VP2 einen späteren Transkriptionsstart im Leserahmen von VP1 besitzt. Das bedeutet, daß beide Proteine bis auf einen zusätzlichen N-terminalen, etwa 26 kD großen Teil von VP1, identisch sind. Das Nicht-Strukturprotein (NS-1) mit einer Größe von ca. 77 kD ist für die Virusreplikation und Vermehrung nötig. Die Unterteilung des Strukturproteins VP1 im RIDA® Blot in zwei Segmente erlaubt eine genauere Interpretation einer vorhandenen Immunantwort. Nach Erstinfektion werden zu Beginn der Immunantwort neben IgM-Antikörpern im allgemeinen IgG-Antikörper gegen lineare Epitope der Strukturproteine VP1 und VP2 gebildet. Antikörper gegen die linearen Epitope am N-terminalen Ende der Strukturproteine (VP-N im RIDA® Blot) bleiben in der Regel ein Leben lang erhalten. Antikörper gegen die linearen Epitope am C-terminalen Ende der Strukturproteine (VP-C) nehmen im Verlaufe von 6 - 12 Monaten jedoch deutlich ab oder gehen sogar ganz verloren. Eine starke IgG-Reaktivität gegen das VP-C deutet somit auf eine frische oder erst kurz zurückliegende Infektion hin. 12.2. Interpretation Ein negatives Ergebnis im Immunoblot kann eine Infektion mit Parvovirus B19 nicht ausschließen. Zu einem sehr frühen Zeitpunkt der Infektion kann die Immunantwort noch so niedrig ausfallen, daß ein serologischer Nachweis nicht möglich ist. In diesem Fall sollte bei bestehendem klinischen Verdacht ebenso wie bei einem fraglichen Ergebnis im Immunoblot nach einer Woche ein Folgeserum RIDA® Blot Parvovirus B19 03-11-11 15 untersucht werden. Ist dann keine deutliche Serokonversion zu sehen, ist eine Parvovirus B19-Infektion mit großer Wahrscheinlichkeit auszuschließen. Struktur des Parvovirus-Genoms: 5’ 3’ NS-1 VP1 VP2 im RIDA Blot verwendete Antigene: VP-N NS-1 VP-1S VP-C Abb.1: Struktur des Parvovirus-Genoms und rekombinant hergestellte Antigene Bei einem positiven oder schwach positiven Befund im IgM-Nachweis sollte grundsätzlich auch der IgG-Befund zur Interpretation herangezogen werden. Neben den Banden VP-N und VP-1S reagiert bei einer Frischinfektion in der Regel auch die Bande VP-C stark. Falls keine IgG-Reaktivität gegen VP-C vorhanden ist, kann eine frische Infektion mit großer Wahrscheinlichkeit ausgeschlossen werden. Eine schwache IgM-Reaktivität kann dann durch persistierende IgM-Antikörper einer schon länger zurückliegenden Infektion, durch reaktivierte IgM-Antikörper z. B. bei einer EBV-Infektion oder durch sich unspezifisch anlagernde Antikörper verursacht werden. Eine deutliche IgG-Reaktivität gegen VP-C bei negativem IgM-Befund deutet auf einen kurz zurückliegenden (höchstens 6 - 12 Monate) Infektionszeitpunkt hin. Eine Reaktivität gegen das NS-1 sollte nur bei bestimmten Fragestellungen in die Interpretation mit einbezogen werden. Bei der Abklärung unklarer Arthropathien zum Beispiel kann der Nachweis von Antikörpern gegen dieses Protein ein Hinweis auf eine persistierende Parvovirus B19-Infektion sein. Da diese Antikörper erst sechs bis acht Wochen nach Infektion nachweisbar sind, deuten sie auf ein 16 RIDA® Blot Parvovirus B19 03-11-11 persistierendes Krankheitsgeschehen hin und lassen in einem gewissen Rahmen Rückschlüsse auf den Infektionszeitpunkt zu. Da Antikörper gegen das NS-1 auch nach überstandener Infektion noch vorhanden sein können (in einer Studie wurde bei 24,7 % der Seren eine teilweise allerdings sehr schwache Reaktivität gegen das NS-1 gefunden), ist der Nachweis dieser nicht als Beweis für eine Persistenz ausreichend. Deshalb sollte bei entsprechendem klinischen Verdacht der Nachweis von Parvovirus-Antigen oder -DNA zur Sicherung der Diagnose herangezogen werden. Hierbei ist zu berücksichtigen, daß eine PCR-Bestimmung nicht zu jedem Zeitpunkt eines persistierenden Krankheitsverlaufes positiv ausfallen muß. Bei der Beurteilung der Reaktivität gegen das NS-1 ist zu beachten, daß in Abhängigkeit von der individuellen Immunantwort auch Antikörper gegen das NS-1 verzögert auftreten können. 12.3. Typische Reaktionsprofile im RIDA® Blot Parvovirus B19 Aufgrund bisher durchgeführter Evaluierungen können die folgenden IgM/IgG-Reaktionsmuster einen Hinweis auf einen bestimmten Parvovirus B19-Status geben. Es muß darauf hingewiesen werden, daß es sich hierbei um typische Reaktionsmuster handelt, von denen es durchaus Abweichungen geben kann. Tabelle 7: Parvovirus B19-Status und typische Antikörpermuster IgM IgG möglicher B19-Status negativ VP-N eindeutig reaktiv, evtl. auch VP-1S; VP-C sehr schwach oder negativ lange zurückliegende Infektion (Jahre) negativ, fraglich oder schwach positiv VP-N und VP-C stark reaktiv, evtl. auch VP-1S Status nach Infektion (Monate) VP-N und VP-C deutlich reaktiv VP-N und VP-C stark reaktiv, evtl. auch VP-1S Status nach Infektion (Wochen) VP-N und VP-C deutlich reaktiv negativ, fraglich oder schwach positiv Status zu einem frühen Zeitpunkt der Infektion VP-N und/oder VP-C (evtl. VP-1S) schwach oder fraglich reaktiv VP-N und VP-C schwach unklarer Status, evtl. reaktiv verursacht durch unspezifische Reaktivierung; Test sollte im zeitlichen Verlauf wiederholt werden RIDA® Blot Parvovirus B19 03-11-11 17 Achtung! Die Bewertung von Titern gegen das NS-1 zur Abklärung persistierender Parvovirus B19-Infektionen, reaktiven Arthropathien, chronischen Anämien oder anderer Symptomatik mit Verdacht auf eine B19-Persistenz wurde in der o. a. Tabelle nicht berücksichtigt, da hier abhängig von Dauer, Klinik und Immunkompetenz eine Vielzahl von Kombinationen möglich ist. Weiterhin kann ein entsprechender Titer nur in Zusammenhang mit der klinischen Symptomatik beurteilt werden. Die Diagnose muß durch einen positiven Antigen- oder Genom-Nachweis abgesichert werden. 13. Leistungsmerkmale 13.1. Vergleichsdaten mit einem kommerziell erhältlichen ELISA Tab. 8: IgG-Vergleich RIDA® Blot Parvovirus B19 IgG negativ (%) fraglich (%) positiv (%) gesamt (%) IgG-ELISA negativ (%) 7 (7,8) 0 (0,0) 0 (0,0) 7 (7,8) fraglich (%) 4 (4,4) 0 (0,0) 6 (6,7) 10 (11,1) positiv (%) 5 (5,6) 1 (1,1) 67 (74,4) 73 (81,1) gesamt (%) 16 (17,8) 1 (1,1) 73 (81,1) 90 (100,0) Tab. 9: IgM-Vergleich RIDA® Blot Parvovirus B19 IgM negativ (%) fraglich (%) positiv (%) gesamt (%) IgM-ELISA 18 negativ (%) 34 (37,8) 2 (2,2) 0 (0,0) 73 (81,1) fraglich (%) 5 (5,6) 1 (1,1) 0 (0,0) 10 (11,1) positiv (%) 9 (10,0) 4 (4,4) 35 (38,9) 7 (7,8) gesamt (%) 48 (53,3) 7 (7,8) 35 (38,9) 90 (100,0) RIDA® Blot Parvovirus B19 03-11-11 13.2. Zeitpunkt des Auftretens von Antikörpern gegen das NS-1 Für diese Fragestellung wurden 82 Serumproben von Frauen mit einer Parvovirus B19-Infektion während der Schwangerschaft untersucht. Die Probennahme lag zwischen zwei Wochen und neun Monaten nach Infektion. In allen Fällen konnte das typische Reaktionsmuster (VP-N und VP-C im IgG stark reagierend, IgM zeitweise positiv) gefunden werden. IgM-Titer gegen das NS-1 traten in keinem Fall auf. IgG-Titer gegen das NS-1 wurden frühestens sechs Wochen nach Infektion gefunden. Diese traten in 32% der untersuchten Fälle auf. 13.3. Häufigkeit von IgG-Titern gegen das NS-1 in der Normalbevölkerung 197 Proben von Blutspendern und 300 Proben von Frauen (getrennt nach Altersgruppen) wurden auf IgG-Titer gegen das NS-1 untersucht. Tabelle 10: Häufigkeit von IgG-Titern Blutspender 20 - 29 J. 30 - 39 J. 50 - 59 J. Anzahl der Seren gesamt 197 99 101 100 497 B19 positiv 75,1% 64,6% 62,3% 69,0% 69,2% NS-1 positiv * 27,7% 37,7% 30,1% 2,9% 24,7% * auch sehr schwache Reaktivitäten wurden in die Auswertung mit einbezogen RIDA® Blot Parvovirus B19 03-11-11 19 RIDA® Blot Parvovirus B19 Immunoblot with recombinant antigens for the detection of antibodies (IgM/IgG) against the human parvovirus B19 1. Intended use For in vitro diagnostic use. The RIDA® Blot Parvovirus B19 is a qualitative in-vitro test for the detection and identification of antibodies (IgM and IgG) against the parvovirus B19 in human serum or plasma. Due to the electrophoretic separation of recombinant components of the virus protein, this test procedure, in contrast to others, allows a statement about the presence of different antibodies which in return can be correlated to the different stages of the illness. 2. General The human parvovirus B19 was discovered by Cossart and co-workers in England in 1975. They discovered the virus while screening the sera of blood donors for hepatitis B. They named this accidentally found isolate B19. The parvovirus B19 is a small, non-enveloped DNA virus with a diameter of 18 26 nm. The genome consists of single-stranded DNA with a length of 5.4 kb. The capsid consists of two polypeptide proteins of about 84 and 58 kD (VP1 and VP2). Both structural proteins are encoded in a common reading frame on the viral genome, whereby the shorter VP2 has a later transcription start in the reading frame of the VP1 (see pt. 12). This means that both proteins are identical, except for one additional N-terminal part of VP1 which has a size of approximately 26 kD. Furthermore, a „main-non-structure protein“ (NS-1) is encoded in the genome; it is necessary for the virus replication and multiplication. The B19 virus has an icosaedrical structure and is very heat-stable. It can sustain a temperature of 60°C for up to 12 h. The genus of the parvoviruses comprises - beside the only known human parvovirus B19 - animal pathogens like the canine parvovirus and the feline panleukopenia virus. Together with the denso viruses and the dependo viruses, that need 20 RIDA® Blot Parvovirus B19 03-11-11 helper viruses (adeno or herpes viruses) for replication, the parvoviruses form the family of parvoviridae. One significant characteristic of the parvoviruses is their ability to selectively replicate in self-dividing cells such as bone marrow, intestinal and embryonic cells. Infections with the worldwide distributed human parvovirus B19 occur more frequently during the winter and early summer seasons. It may arise to epidemic outbreaks especially in day care and schools. The transmission is mainly caused via the respiratory system (droplet infection), but it can also be transmitted by blood and blood products. Parvovirus infections occur in all age groups, but are most common between the ages of 6 and 15 years. The prevalence increases with age and reaches a value of 40 - 70% for adults. Women show a higher prevalence than men. The incubation time lasts 1 - 3 weeks. The viremic phase in which the patient is considered infectious, is limited to 3 - 7 days. During this time, the patient can be asymptomatic or he can complain about some prodromal illnesses such as headache, itchiness, myalgia and fever. Approximately two weeks after infection, an erythema infectiosum (fifth disease) can occur. Children usually show typical exanthemas (redness of cheeks, lattice-like febrile purpura especially along the extensor surfaces of the extremities), but these are rather untypical for adults. Further symptoms of a B19 infection are arthralgias and arthritis (60%), respiratory symptoms (22%) as well as diarrhea (15 - 35%). Only approximately 20% of all parvovirus B19 infections are symptomless. Women are affected by joint pain twice as much as men. In most cases, the arthropathies disappear within two to four weeks. In a few cases, the symptoms can persist intermittently over years. So that if chronic arthropathies should be verified, a persistent parvovirus B19 infection must also be considered. The inhibition of erythropoiesis (duration 1 - 4 weeks), which is caused by parvovirus B19, usually remains subclinical in healthy persons, but it can cause an aplastic crisis in patients with chronic hemolytic anaemia (sickle cell anaemia, thalassaemia, pyruvate kinase deficiency, spherocytosis, autoimmune hemolytic anaemia). Such patients require transfusions and should be submitted to a hospital. Additional organ manifestations such as hepatic dysfunctions or a B19 associated myocarditis have also been reported recently. A further complication following a B19 infection can occur in sero-negative pregnant women. The parvovirus B19 can be transmitted via the placenta to the fetus. Due to the short viability of the erythrocytes up to the 20th week of pregnancy and a missing efficient immune defense, an infection can lead to a severe acute or chronic anaemia and subsequent spontaneous abortion. A further complication after infection during the second trimenon, is the development of a hydrops fetalis. However, more than 80% of the pregnancies course without complications. Embryopathies have not been observed so far. RIDA® Blot Parvovirus B19 03-11-11 21 Antibodies of the IgM group can be detected approximately 10 days after the infection and usually occur with the beginning of the symptoms. IgG antibodies can already be found some days later and usually remain for life. However, IgM antibodies cannot be detected after 30 - 60 days. Elisa systems, on the basis of recombinant VP1/VP2 peptides, are suitable for the detection of such antibodies. Because of a more specific statement regarding the possible stages of the illness, due to the detection of different antibodies, a Western Blot such as the RIDA® Blot Parvovirus B19, which uses different recombinantly produced proteins of the virus antigen, should always be used additionally. 3. Test principle The RIDA® Blot Parvovirus uses four recombinant parvovirus B19 antigens, which are produced in E. coli. This involves parts of the two structural proteins, VP1 and VP2, and the „main-non-structure protein“ NS-1 (see pt. 12.). The cleaned (free of fusion proteins), recombinant antigens were electrophoretically separated by molecular weight and blotted onto a nitro-cellulose membrane. Following that, the membrane was cut into individual blot strips. These strips are incubated with the sample (serum or plasma) that is to be examined. During incubation, the specific antibodies present in the sample will bind to the corresponding protein bands. After removal of unbound antibodies by a washing step, a second incubation with anti-human IgM or IgG conjugate (peroxidase) and subsequent color reaction, specifically bound antibodies against the four antigens of parvovirus B19 become visible as blue bands on the strips. 4. Reagents provided The reagents are sufficient for 20 determinations. Each test kit contains: 2 x 10 Teststrips; coated with recombinant antigens of parvovirus B 19 1 x Washing / Dilution Buffer (100 ml, 5x conc.); contains Tris buffer, NaCl, Tween-20 and protein 1 x Low Positive IgM Control (80 µl); red cap human serum, contains < 0,1 % NaN3 1 x Low Positive IgG Control (80 µl); white cap human serum, contains < 0,1 % NaN3 1 x Negative Control (80 µl); blue cap human serum, contains < 0,1 % NaN3 22 RIDA® Blot Parvovirus B19 03-11-11 1 x Anti-human IgM Conjugate (100 µl, 500x conc.); rabbit, horseradish peroxidase conjugated, contains < 0,1 % NaN3 1 x Anti-human IgG Conjugate (60 µl, 1000x conc.); rabbit, horseradish peroxidase conjugated, contains < 0,1 % NaN3 1 x Substrate (45 ml); ready to use, contains tetramethylbenzidine (TMB) 2 x Incubation plates with 10 chambers each 1 x Control strip (developed, specific for the kit) 1 x Instructions for use 2 x Protocol sheets violet cap green cap 5. Materials required but not provided 5.1. Reagents − Deionized water 5.2. Accessories − Vacuum pump to remove liquid out of the incubation chambers − Pipets for 2 - 10 µl, 10 - 100 µl and 2 ml − Measuring cylinder for 100 ml and 500 ml − Shaker − Plastic tweezers to handle the strips 6. Warnings and precautions for the users For in vitro diagnostic use only. The test has to be used only by experienced laboratory staff. Please refer to guidelines for safety regulations in medical laboratories. The test protocol must be followed strictly. Do not mouth pipette samples or reagents. Avoid contact with injured skin or mucous membranes. Wear disposable gloves while handling samples and wash hands after assay is complete. Do not smoke, eat or drink in areas where specimen or kit reagents are handled. The control sera (Positive and Negative Control) of the kit have been tested for HIV 1+2- and HCV-Ab as well as for HBsAg and were found to be negative. How- RIDA® Blot Parvovirus B19 03-11-11 23 ever, the controls as well as the patient samples should be considered potentially infectious and be treated with respect to the given national safety precautions. The conjugates and the controls contain NaN3. Contact with skin or mucous membranes should be avoided. Contact with lead or copper pipes can form explosive metal azides. All reagents and materials coming in contact with potential infectious specimens must be treated with disinfectants or autoclaved at 121°C for at least one hour. 7. Storage instructions All reagents have to be stored at 2 - 8°C and can be used up to the expiry date printed on the labels. Reagents from kits with different lot numbers should not be interchanged. Microbial contamination has to be avoided. The concentrated conjugates and the buffer have to be diluted freshly in required amounts. 8. Indication of instability or deterioration of reagents Deterioration of reagents can be indicated by a missing reaction of the incubation control or absence of bands with the Positive Controls so that they do not comply with the criteria shown in point 11. The packages have an expiry date after which a quality warranty cannot be given. 9. Specimen collection and storage The RIDA® Blot Parvovirus B19 can be carried out with serum or plasma. Heat inactivated samples can lead to higher background reactions. Repeated freezing and thawing of the samples as well as microbial contamination must be avoided. The application of lipemic, hemolytic or turbid samples can cause a dark background coloration of the strips. Furthermore, these samples can lead to false results and should not be used. The samples can be stored for up to 2 weeks at 2 - 8°C if the test cannot be carried out immediately. A prolonged storage of samples is possible at -20°C. 10. Test procedure 10.1. Preliminary comments Bring all kit components to room temperature prior to use for at least 30 minutes. The vial containing the strips should be opened thereafter to avoid formation of condensed water. The strips that are not required remain in the vial and continue 24 RIDA® Blot Parvovirus B19 03-11-11 to be stored at 2 - 8°C (vial should be closed tightly, strips have to remain dry prior to use!). Remove only the volume of reagents that is needed for test procedure. Do not pour reagents back into vials as reagent contamination may occur. Strips and reagents must not be used if pouch is damaged or vials are leaking. The strips do not have to be used in their order of numeration. But it is important to keep a record about which strip is incubated with the corresponding sample. The reproducibility of the Western Blot results depend very strongly on the consistency of washing the strips. The washing steps described below should always be adhered to. Attention! The small test tubes should be centrifuged for a short time before opening, so that the liquid can collect on the bottom of the tube and nothing is lost. 10.2. Preparation of the ready to use Washing / Dilution Buffer The concentrated buffer contains soluble protein. Prior to use, it should be shaken to ensure a homogenous dispersion. The buffer is used for the sample dilution, and the preparation of conjugate solutions. The Washing / Dilution Buffer has always to be prepared freshly. The required volume for the corresponding number of tests must be determined. The diluted Washing / Dilution Buffer is not stable. Unused buffer must be disposed of. One part of concentrated buffer is diluted with four parts deionized water (dilution 1:5). Table 1: Washing-/Dilution Buffer per applied strip applied strips concentrated Washing / Dilution Buffer deionized water ready to use buffer 2 5 10 15 20 10 ml 25 ml 50 ml 75 ml 100 ml 40 ml 100 ml 200 ml 300 ml 400 ml 50 ml 125 ml 250 ml 375 ml 500 ml 10.3. First Incubation For each determination, use one chamber of the incubation plate and fill it with 2 ml diluted Washing / Dilution Buffer. For each determination, one blot strip is RIDA® Blot Parvovirus B19 03-11-11 25 taken out of the vial with a pair of tweezers (touch the strips at the end with the numeration only). Dip the strips into the buffer. The strips must be completely wetted with buffer. The strip numeration must show upwards. 20 µl of the undiluted sample (serum or plasma) or of the respective Low Positive Controls and of the Negative Control are added to the corresponding chambers. The Low Positive Controls must be carried out with each test run, independent on the number of sera to be tested. It must be taken care that the neighboring chambers are not contaminated since this could lead to false positive results. During the incubation, the incubation plates should be covered up with the lids that are enclosed in the test kit. The blot strips with the sample are placed on a horizontal shaker and are incubated overnight (10 to 16 hours) at room temperature (18 - 25°C). 10.4. Washing Remove the solution (via suction), preferably with an attached disinfection trap. Wash the strips for 5 min by addition of 2 ml diluted Washing / Dilution Buffer to each strip. Place the incubation plate on the shaker. Repeat the procedure three times. Between the washing steps, the buffer is sucked out of the chambers. Attention! The conjugate solution must be prepared during the last washing step. 10.5. Preparation of the conjugate solution The conjugate enclosed in the kit is provided as a concentrate. For its application to the test, it must be diluted with the ready to use Washing / Dilution Buffer. Since the diluted conjugate is stable only for a limited period of time, it must be prepared freshly prior to its application. 10.5.1. IgM conjugate For the determination of IgM antibodies, a 1:501 dilution must be prepared with the Anti-human IgM Conjugate enclosed in the kit. The required volumes for the corresponding number of strips are listed in Table 2. 26 RIDA® Blot Parvovirus B19 03-11-11 Table 2: Preparation of the ready to use IgM conjugate solution applied strips concentrated Anti-human IgM Conjugate ready to use Washing / Dilution Buffer 2 4 8 16 20 10 µl 20 µl 40 µl 80 µl 100 µl 5 ml 10 ml 20 ml 40 ml 50 ml 10.5.2. IgG conjugate For the determination of IgG antibodies, a 1:1001 dilution must be prepared with the Anti-human IgG Conjugate enclosed in the kit. The required volumes for the corresponding number of strips are listed in Table 3. Table 3: Preparation of the ready to use IgG conjugate solution applied strips concentrated Anti-human IgG Conjugate ready to use Washing / Dilution Buffer 2 4 8 16 20 5 µl 10 µl 20 µl 40 µl 50 µl 5 ml 10 ml 20 ml 40 ml 50 ml 10.6. Second incubation Add 2 ml of the corresponding ready to use conjugate solution to each strip. Incubate the strips for one hour on a horizontal shaker at room temperature. 10.7. Washing Washing sequence: see point 10.4. 10.8. Third incubation Add 2 ml of the ready to use Substrate solution to each strip. Incubate the strips for 5 - 15 min at room temperature, until the intensity of the bands of the Low Positive Controls is complying to the criteria given in point 11. Thereafter, the Substrate is removed via suction. Still in their chambers, the strips should be rinsed three times with deionized water to stop the color reaction. RIDA® Blot Parvovirus B19 03-11-11 27 The strips are carefully taken out of the chambers with tweezers. To dry the strips, they are placed between filter paper. After drying they can be evaluated. Attention! Highly positive sera can induce an overshooting color reaction. It is recommended to stop the reaction prematurely with these sera Summary of the test procedure 1. Bring all reagents to room temperature 2. Pipet 2 ml Washing / Dilution Buffer into each chamber 3. Place one strip into each chamber 4. Add 20 µl sample, Low Positive or Negative Control 5. Incubate overnight at room temperature (10 - 16 h) 6. Wash 4 times with 2 ml Washing / Dilution Buffer; 5 min each time 7. Add 2 ml freshly prepared conjugate solution 8. Incubate for 1 hour at room temperature 9. Wash 4 times with 2 ml Washing / Dilution Buffer; 5 min each time 10. Add 2 ml Substrate 11. Incubate for 5 - 15 min at room temperature 12. Rinse strips with deionized water 13. Dry on filter paper 14. Analysis 11. Analysis The function of the testkit is checked by Low Positive Controls which have to be included in each test procedure, by the Negative Control and by the incubation control band that is present on each strip. The incubation control band can be found below the numeration. It consists of protein A which binds globulins and must, therefore, be visible on each strip if the test performance is correct. With correct test performance, the Low Positive IgG Control should show a weak VP-N band, but clearly visible; VP-C shows a much weaker and relatively wide and diffuse band. The VP-1S band reacts only very weak or not at all with this serum. 28 RIDA® Blot Parvovirus B19 03-11-11 With the Low Positive IgM Control, the VP-N band is relatively clearly visible and the VP-C band only very weak. The Negative Control should show no other band except for the incubation control band. If the expected conditions are not fulfilled please check the following before repeating the test: − expiration date of the reagents − calibration of the used instruments − exact test procedure − visual examination of kit components for signs of contamination or leakage If the conditions are not fulfilled after repeating, please contact your local distributor of R-Biopharm. For better documentation, the strips can be taped to the enclosed protocol sheets and the identified bands can be recorded. The protocol sheets should include the date and the lot number. To analyze the patient sample, the incubation control band of the test strip has to be aligned with the control band of the strip on the evaluation template. With the help of the band descriptions on the evaluation template, the visible bands of the patient samples can be identified. The intensity of the identified bands is compared to the intensity of the bands on the strips with the corresponding Low Positive Controls (IgM or IgG). With this comparison and with the following table, the intensity of the individual bands is determined and recorded on the protocol sheet. Table 4: Analysis of the band intensity Band intensity Evaluation - invisible +/- very weak intensity + weak intensity (comparable to the Low Positive Control) visible intensity ++ strong intensity +++ 11.1. Analysis of IgM detection For the positive/negative analysis of the IgM detection, a possibly existing reactivity of antibodies against the NS-1 protein is not taken into consideration. RIDA® Blot Parvovirus B19 03-11-11 29 Table 5: IgM-Analysis IgM positive and VP-N at least + VP-C at least +/- other bands can, but don’t have to appear IgM questionable or or VP-N at least + VP-C at least + VP-N and VP-C +/- IgM negative no reaction or other constellations other bands can, but don’t have to appear 11.2. Analysis of IgG detection For the positive/negative analysis of the IgG detection, a possibly existing reactivity of antibodies against the NS-1 protein is not taken into consideration. Table 6: IgG-Analysis IgG positive VP-N at least + other bands can, but don’t have to appear IgG questionable IgG negative VP-C at least + VP-N and VP-C +/- no reaction or or other constellations, other bands can, but don’t especially weak isolated reactions against VP-1S have to appear 11.3. Analysis of reactivity against NS-1 Today’s level of knowledge shows that antibodies against this protein only appear with persistent parvovirus B19 infections. Therefore, a reactivity against the NS-1 is not considered for a positive evaluation of the Western Blot. So far, only IgG antibodies against the NS-1 have been identified. At the earliest, they were found six to eight weeks after infection occurs. An existing reactivity against the NS-1 can thus be considered as indicative for a possibly persistent infection. 12. Remarks about the test procedure and interpretation 12.1. Diagnostic significance of recombinant B19 antigens The parvovirus B19 genome with a size of approximately 5.4 kb contains the genetic information of two structural proteins and one non-structure protein (see fig.1). The capsid which envelops the DNA is formed with the two structural proteins VP1 and VP2. Both structure proteins with a size of 84 kD and 58 kD are en30 RIDA® Blot Parvovirus B19 03-11-11 coded on the common reading frame of the viral genome, whereby the smaller VP2 has a downstream transcription start on the reading frame of VP1. This means that both proteins are identical except for an additional N-terminal sequence on VP1 which has a size of 26 kD. The non-structure protein (NS-1) with a size of approximately 77 kD is necessary for the virus replication and multiplication. In the RIDA® Blot, the structure protein VP1 is subdivided into two segments which allow an exact interpretation of an existing immune response. After an initial infection, at the beginning of the immune response, IgM antibodies and usually also IgG antibodies are formed against linear epitopes of the structure proteins VP1 and VP2. Antibodies formed against the linear epitopes at the end of the Ntermini of the structure proteins (VP-N in the RIDA® Blot) usually remain for life. Antibodies formed against the linear epitopes on the end of the C-termini of the structural proteins (VP-C) are significantly reduced within 6 - 12 months or disappear altogether. A strong reactivity against the VP-C, therefore, indicates a fresh or just recently obtained infection. Structure of the Parvovirus genome: 5’ 3’ NS-1 VP1 VP2 Antigens used in the RIDA Blot: VP-N NS-1 VP-1S VP-C Fig. 1: Structure of the Parvovirus genome and recombinant antigens 12.2. Interpretation A negative result in the immunoblot does not exclude an infection with parvovirus B19. Very early, at the beginning of the infection, the immune response can be so weak, that a serological detection is not possible. In this case, if a clinical suspiRIDA® Blot Parvovirus B19 03-11-11 31 cion persists or if the result of the immunoblot is questionable, a consecutive serum should be examined after one week. If a distinct seroconversion is not visible, a parvovirus B19 infection is not likely. If the result in the IgM detection is positive or weakly positive, the IgG result should always also be taken into consideration. In addition to the bands VP-N and VP-1S, the band VP-C usually also reacts very strongly if infection is fresh. If an IgG reactivity against VP-C is not present, a fresh infection is not likely. A weak IgM reactivity can be caused by persistent IgM antibodies of a previous infection by reactivated IgM antibodies, e.g. after an EBV-infection, or by unspecifically bound antibodies. A distinct reactivity against VP-C with negative IgM result indicates a recent infection (6 - 12 months). A reactivity against the NS-1 should only be included if specific questions need to be clarified. For example, if uncertain arthropathies have to be clarified, the detection of antibodies against this protein can be indicative for a persistent parvovirus B19 infection. Since these antibodies are only detectable six to eight weeks after the infection, they indicate a persistent illness and allow some conclusions about the onset of infection to be drawn. Since antibodies against NS-1 can be present even when the infection has passed (in a study, 24.7 % of the sera showed a partially very weak reactivity against NS-1), thus this reaction is not a sufficient proof of a persistent infection. Therefore, in case of clinical suspicion, the detection of parvovirus antigens or DNA should be considered for a secure diagnosis. It must be considered that a PCR-determination is not necessarily positive at each moment of the development of a persistent illness. When the reactivity of NS-1 is evaluated, it must be considered that with regard to the individual immune response, antibodies against NS-1 can also appear with delay. 12.3. Typical reaction profiles in the RIDA® Blot Parvovirus B19 Due to evaluations that have been carried out so far, the following IgM/IgG reaction patterns can be an indication of a specific parvovirus B19 status. It must be pointed out that this involves typical reaction patterns, but they can also show deviations. 32 RIDA® Blot Parvovirus B19 03-11-11 Table 7: parvovirus B19 status and typical antibody patterns IgM IgG possible B 19 status negative VP-N clearly reactive, infection occurred long possibly also VP-1S; time ago (years) VP-C very weak or negative negative, questionable or weakly positive VP-N and VP-C strongly reactive, possibly also VP-1S status after infection (months) VP-N and VP-C clearly reactive VP-N and VP-C strongly reactive, possibly also VP-1S status after infection (weeks) VP-N and VP-C clearly reactive negative, questionable or status of an early infection weakly positive VP-N and/or VP-C (possibly VP-1S) weak or questionably reactive VP-N and VP-C weakly reactive unclear status, possibly caused by unspecific reactivation; test should be repeated in time Attention! The analysis of titers against the NS-1 was not considered in the above table for the clarification of persistent parvovirus B19 infections, reactive arthropathies, chronic anaemias or other symptoms with suspicion of a B19 persistence, since depending on the duration, the clinic and the immunocompetence, numerous combinations are possible. Furthermore, a corresponding titer can only be evaluated in combination with clinical symptomatic. The diagnosis must be secured with a positive antigen or genome detection. RIDA® Blot Parvovirus B19 03-11-11 33 13. Clinical results 13.1. Comparative data with a commercial available ELISA Table 8: IgG data RIDA® Blot Parvovirus B19 IgG negative (%) equivocal (%) positive (%) total (%) IgG-ELISA negative (%) 7 (7.8) 0 (0.0) 0 (0.0) 7 (7.8) equivocal (%) 4 (4.4) 0 (0.0) 6 (6.7) 10 (11.1) positive (%) 5 (5.6) 1 (1.1) 67 (74.4) 73 (81.1) total (%) 16 (17.8) 1 (1.1) 73 (81.1) 90 (100.0) Table 9: IgM data RIDA® Blot Parvovirus B19 IgM negative (%) equivocal (%) positive (%) total (%) IgM-ELISA negative (%) 34 (37.8) 2 (2.2) 0 (0.0) 73 (81.1) equivocal (%) 5 (5.6) 1 (1.1) 0 (0.0) 10 (11.1) positive (%) 9 (10.0) 4 (4.4) 35 (38.9) 7 (7.8) total (%) 48 (53.3) 7 (7.8) 35 (38.9) 90 (100.0) 13.2. Time of occurrence of antibodies against the NS-1 For clarification of this question, 82 serum samples of women with parvovirus B19 infection during pregnancy were examined. Samples were taken between two weeks and nine months after infection. In all samples, the typical reaction pattern could be found (VP-N and VP-C in IgG strongly reactive, IgM temporarily positive). IgM titer against NS-1 did not appear in any sample. IgG titer against the NS-1 were found at the earliest six weeks after infection. These appeared in 32 % of the examined samples. 13.3. Frequency of IgG titers against the NS-1 in the normal population 197 samples of blood donors and 300 samples of women (separated in age groups) were examined for IgG titers against NS-1. 34 RIDA® Blot Parvovirus B19 03-11-11 Table 10: Frequency of IgG titers Blood donors 20-29 yrs. 30-39 yrs. 50-59 yrs. Number of sera total 197 99 101 100 497 B19 positive 75.1 % 64.6 % 62.3 % 69.0 % 69.2 % NS-1 positive * 27.7 % 37.7 % 30.1 % 2.9 % 24.7 % * also very weak reactivities were included in the analysis Appendix Literature 1. Marshall, B. F., Royce, H., Annear, D. I., Goodwin, C. S., Taylor, N. S., Edmonds, P., Sly, L. I., Brenner, D. J.: Original Isolation of Campylobacter pyloridis from human gastric mucosa. Microbios Letter 25, 83 (1982) 2. Warren, J. R.: Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet I, 1273 - 1275 (1983) 3. Parsonnet, J., Friedman, G. D., Vanderstetten, D. P., Chang, Y., Vogelman, J. H., Orentreich, N., Sibley, R. K.: Helicobacter pylori infection and the risk of gastric carcinoma. N. Engl. J. Med. 325, 1127 - 1131 (1991) 4. Stolte, M., Eidt, S.: Healing gastric MALT lymphomas by eradicating H. pylori. Lancet 342, 568 (1993) 5. Stolte, M.: Helicobacter pylori and gastric MALT lymphoma. Lancet 339, 745 - 746 (1992) 6. Hentschel, E., Brandstatter, G., Dragosics, B., Hirschl, A. M., Nemec, H., Schutze, K., Taufer, M., Wurzer, H.: Effect of Ranitidine and Amoxicillin plus Metronidazole on the eradication of Helicobacter pylori and the recurrence of duodenal ulcer [see comments]. N. Engl. J. Med. 328, 308 - 312 (1993) 7. Stadelmann, O.: Helicobacter pylori: Indikationen und Praxis der Therapie. Deutsches Ärzteblatt 92, 39 - 41 (1995) 8. Telford, J. L., Ghiara, P., Dellorco, M., Comanducci, M., Burroni, D., Bugnoli, M., Tecce, M. F., Censini, S., Covacci, A., Xiang, Z. Y., Papini, E., Montecucco, C., Parente, L., Rappuoli, R.: Gene structure of the Helicobacter pylori cytotoxin and evidence of ist key role in gastric disease. J. Exp. Med. 179, 1653 -1658 (1994) RIDA® Blot Parvovirus B19 03-11-11 35 9. Lee, A.: H. pylori initiated ulcerogenesis: look to the host. Lancet 341, 281 (1993) 10. Schmitt, W., Haas, R.: Genetic analysis of the Helicobacter pylori vacuolating cytotoxin - structural similarities with the IgA protease type of exported protein. Mol. Microbiol. 12, 307 - 319 (1994) 11. Covacci, A., Censini, S., Bugnoli, M., Petracca, R., Burroni, D., Macchia, G., Massone, A., Papini, E., Xiang, Z., Figura, N., Rappuoli, R.: Molecular characterization of the 128-kDa immunodominant antigen of Helicobacter pylori associated with cytotoxicity and duedenal ulcer. Proc. Natl. Acad. Sci. USA 90, 5791 - 5795 (1993) 12. Xiang, Z., Censini, S., Bayeli, P. F., Telford, J. L., Figura, N., Rappuoli, R.: Analysis of expression of cagA and vacA virulence factors in 43 strains of Helicobacter pylori reveals that clinical isolates can be divided into two major types and that cag A is not necessary for expression of the vacuolating cytotoxin. Infect. Immun. 63, 94 (1995) 13. Krakowka, S., Morgan, D. R., Kraft, W. G., Leunk, R. D.: Establishment of gastric Campylobacter pylori infection in the neonatal gnotobiotic piglet. Infect. Immun. 55, 2789 - 2796 (1987) 14. Karita, M., Li, Q., Cantero, D., Okita, K.: Establishment of a small animal model for human Helicobacter pylori infection using germ-free mice. Am. J. Gastroenterol. 89, 208 - 213 (1994) 15. Marchetti, M., Arico, B., Burroni, D., Figura, N., Rappuoli, R., Ghiara, P.: Development of a mouse model of Helicobacter pylori infection that mimics human disease. Science 267, 1655 - 1658 (1995) 16. Jaskowski, T. D., Martins, T. B., Hill, H. R., Litwin, C. M.: Immunoglobulin A Antibodies to Helicobacter pylori. J. Clin. Microbiol. 35, 2999 - 3000 (1997) 36 RIDA® Blot Parvovirus B19 03-11-11