Hepatitis C – Genotyp 3 richtig behandeln
Werbung

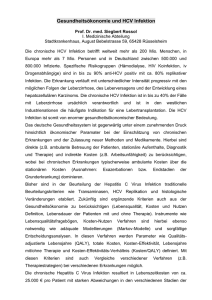
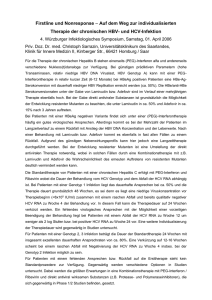
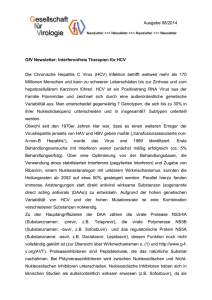
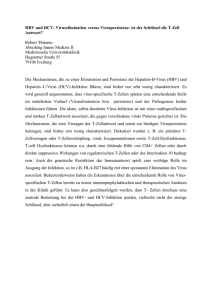
Hepatitis C – Welche Behandlung für Genotyp 3? HCV GT-3 ist der zweithäufigste Genotyp weltweit Schätzungsweise 54.3 Millionen Patienten sind weltweit mit HCV GT3 infiziert UK Canada 47% 22% China Germany 4% 28% France 20% US 12% Japan Spain 1% 20% Brazil 30% Argentina 18% GT-3 Other Australia 31% Pakistan 68% India 71% 1. Messina et al. Hepatology. 2015;61:77-87. 2. Sievert. Liver Int 2011;31(suppl 2):61. 3. Cornberg. Liver Int 2011;31(suppl 2):30. 4. Kershenobich. Liver Int 2011;31(suppl 2):18. 5. Germer et al. J Clin Microbiol 2011;49:3040. 6. Public Health England. Hepatitis C in the UK. 2013 Report. July 2013. 7. Pawlotsky et al. J Infect Dis 1995;171:1607. 8. Gower, et al. J Hepatol 2014;61:S45-57. Prävalenz der HCV Genotypen in Deutschland Insgesamt leben in Deutschland bis zu 385.000 HCV Patienten, davon sind ca. 28% mit GT-3 infiziert 3% 28% 7% Genotyp 1 62% Genotyp 2 Genotyp 3 Adaptiert nach: Hüppe et al., Epidemiologie der chronischen Hepatitis C in Deutschland; Z Gastroenterol 2007 Genotyp 4/5/6 HCV GT-3 ist mit einer raschen Fibrose-Progression assoziiert Proportion of patients Progression to fibrosis stage F3–F41a 1.00 GT-1 or -4, n = 630 0.80 GT-2, n = 92, p = 0.4 0.60 GT-3, n = 342, p < 0.001 0.40 0.20 0.00 0 5 10 15 20 25 30 35 40 Years infected Beschleunigte Fibrosierung vermutlich u.a. durch zytopathischen Effekt der durch HCV GT-3 induzierten Steatose1,2 a Markov modelling of biopsies and genotypes in 1189 Swiss patients with HCV. 1. Tapper and Afdhal. J Viral Hepat 2013;20:669–77. 2. Leandro et al. Gastroenterology 2006;130:1636–42. GT-3 ist mit dem Auftreten von Steatose assoziiert1 Prevalence of steatosis (% patients) 90 80 82 60 83 80 77 70 GT-3 Other 75 67 63 62 61 61 50 40 47 43 43 36 30 26 20 24 10 0 Hourigan 19992 Rubbia-Brandt 20003 Adinolfi 20014 Westin 20025 Poynard 20036 Castéra 20037 Asselah 20038 Rubbia-Brandt 20049 Steatose vermutlich für beschleunigte Fibrose-Progression sowie niedrige virologische Ansprechraten (sustained virologic response, SVR) verantwortlich1 Figure adapted from 1. Asselah et al. Gut 2006;55:123. 2. Hourigan et al. Hepatology 1999;29:1215–9. 3. Rubbia-Brandt et al. J Hepatol 2000;33:106–15. 4. Adinolfi et al. Hepatology 2001;33:1358–64. 5. Westin et al. J Hepatol 2002;37:837–42. 6. Poynard et al. Hepatology 2003;38:75–85. 7. Castéra et al. Gut 2003;52:288–92. 8. Asselah et al. Gut 2003;52:1638–43. 9. Rubbia-Brandt et al. Gut 2004;53:406–12. Eine erfolgreiche HCV-Behandlung (SVR) reduziert den Schweregrad der Steatose bei GT-3 Patienten Severity of steatosis in pre- and posttreatment liver biopsies using computerassisted morphometric image analysis as well as conventional semiquantitative scoring in 34 patients with GT-3. GT-3: SVR P=0.001 10 8 6 4 2 0 P=0.4 12 Area of Steatosis, % 12 Area of Steatosis, % GT-3: No SVR 10 8 6 4 2 0 Pretreatment Posttreatment Pretreatment Posttreatment • Erfolgreiche Viruseradikation vollständige Rückbildung der hepatischen Steatose • Keine Änderung der Steatose bei GT-3-Patienten, die SVR12 nicht erreichten GT, genotype; SVR, sustained virologic response Kumar et al. Hepatology. 2002;36:1266. Zirrhose-Patienten mit HCV GT-3 Infektion haben ein erhöhtes Risiko der Entwicklung eines Leberzellkarzinoms (HCC) Probability of HCC-free survival according to HCV genotype HCC-free survival 1.0 p = 0.001 0.8 GT-4 0.6 GT-2 GT-1 0.4 0.2 GT-3 0 0 2 4 6 8 Years 10 12 • Höheres HCC-Risiko bei GT-3 unabhängig von bereits bekannten Risikofaktoren inklusive des Steatosegrads • Steatose im GT-3 häufiger, Grad der Steatose nicht mit HCC-Entwicklung assoziiert Retrospective study of 353 patients with cirrhotic HCV in France, prospectively followed and screened for HCC between 1994 and 2007. Log-rank test and Cox model were used to compare the incidence of HCC between genotype subgroups. Nkontchou et al. J Viral Hepat 2011;18:e516–22. Genotyp 3 – Daten aus klinischen Studien und Early Access Programmen VALENCE Phase III Studie: Sofosbuvir + Ribavirin 12 vs 24 Wochen bei behandlungsnaiven und vorbehandelten GT-2 und GT-3 Patienten GT2 und 3; n= 85 Placebo GT2: n=73 GT3: n=11 SOF 400 mg QD + RBV GT3: n=250 Follow-Up SOF 400 mg QD + RBV Tag 1 Woche 12 Woche 24 Select baseline characteristics: • N = 419 • GT 2 (22%); GT 3 (78%) • Previously treated: 58%; 30% non response • 21% with cirrhosis Cirrhosis definition: • Liver biopsy showing cirrhosis • Fiboscan (in countries where locally approved) showing cirrhosis or results >12.5 kPa • FibroTest® score of >0.75 AND an AST:platelet ratio index (APRI) of >2 during Screening GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. Zeuzem S, et al. N Engl J Med. 2014;370:1993-2001. VALENCE: 24 Wochen SOF + RBV bei GT-3 Patienten 24 Weeks SOF + RBV: SVR12 Rates By Treatment Experience in GT-3 Patients Safety: 100 94% 92% 85% SVR12, % 80 20 87% • wenige Therapieabbrüche aufgrund Unerwünschter Ereignisse (AEs) (<1%) 12 27 87 ≥15% der 13 100• häufigste AEs (in45 Patienten): - Kopfschmerzen (30%) - Erschöpfung (30%) Experienced, Experienced, - Juckreiz (27%) Noncirrhotic Cirrhotic - Asthenie (21%) - Übelkeit (13%) - Schlaflosigkeit (16%). 60% 60 40 • 4% schwerwiegende unerwünschte Ereignisse (SAEs), 212 250 86 92 0 Overall Naive, Noncirrhotic Naive, Cirrhotic GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. Zeuzem et al. AASLD 2013. Abstract 1085. HCV-TARGET Register (Real-life Kohorte): SVR12-Raten 100 86% SVR12 (% patients) 80 67% 60 40 20 87/130 12/14 0 105 109 20 32GT-3 SOF + Peg /RBV (12 weeks) 73 75 11 19 32 GT-3 34 SOF + RBV (24 weeks) Relapser 1 7% 36 28% Viral breakthrough 0 0% 2 2% Non-responder 1 7% 0 0% Non-virologic failure 0 0% 5 4% 9 13 Niedrigere SVR12-Raten im Real-life Setting als in Valence Studie GT-3 weiter problematisch GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. Adapted from Welzel et al. AASLD 2015. Poster 1057. HCV-TARGET: SVR12-Raten bei GT-3 Patienten mit SOF + RBV für 24 Wochen 100 SVR12 (%) 80 60 40 20 0 GT-3 Cirrhotic GT-3 Noncirrhotic GT-3 Noncirrhotic TN TE TN TE 16 SVR12 Relapse GT-3 Cirrhotic 212 250 62% 8 31% 0 0% Non-responder 0 Non-virological failure 2 Viral breakthrough 20 86 92 44% 31 12 13 3 86% 20 87% 87 8% 100 2 27 45 9% 1 4% 23 51% 0 0% 0% 0 0% 0 0% 0 0% 8% 2 4% 1 3% 0 0% 1 3% TE, treatment-experienced; TN, treatment-naïve GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. Adapted from Welzel et al. AASLD 2015. Poster 1057. BOSON Studie: SOF + RBV für 16 oder 24 Wochen versus SOF + PEG + RBV für 12 Wochen bei GT-3 Patienten* Patients stratified by cirrhosis HCV genotype and prior HCV treatment n=196 SOF + RBV n=199 n=197 SVR12 SOF + RBV SOF + PEG / RBV Tag 1 SVR12 SVR12 Woche 12 Woche 16 Woche 24 Woche 28 Woche 36 Inclusion criteria: • GT-2- TE with cirrhosis • GT-3- Treatment-naïve and –experienced with or without cirrhosis • Platelets ≥60,000 cells/mm3 * einige GT-2 Patienten eingeschlossen GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. Foster GR. et al. EASL 2015. Abstract L05. BOSON Studie: SVR12 bei GT-3 Patienten stratifiziert nach Vortherapie und Zirrhose-Status SOF + RBV 16 weeks 100 83 90 96 82 91 76 SOF + PEG/RBV 12 weeks 82 94 86 77 57 80 SVR12 (%) SOF + RBV 24 weeks 47 60 Patient population • 92% GT-3 (N=544) • 53% TE • 37% cirrhotic 40 20 105 20 109 32 58 65 68 70 72 71 73 75 12 18 21 21 22 23 11 19 41 44 49 54 54 52 32 9 34 13 17 26 30 36 34 35 0 No Cirrhosis Cirrhosis Treatment Naïve • • No Cirrhosis Cirrhosis Treatment Experienced SOF + RBV schneidet schlecht ab INF in der deutschen Leitlinie nicht empfohlen Error bars represent 95% confidence intervals. GT, genotype; HCV, hepatitis C virus; QD, once daily; RBV, ribavirin; SOF, sofosbuvir; SVR 12, sustained virologic response at posttreatment week 12. Foster GR. et al. EASL 2015. Abstract L05. ALLY-3 Studiendesign: SOF + DCV 12 Wochen bei GT-3 Patienten Open-label GT-3 Therapie-naiv N = 101 DCV 60 mg + SOF 400 mg 1x/tägl. Follow-Up Therapie-erfahren N = 51 DCV 60 mg + SOF 400 mg 1x/tägl. Follow-Up Tag 1 Woche 12 Einschlusskriterien: – Therapienaiv oder –erfahren – Einschließlich Patienten mit kompensierter Zirrhose: - Leberbiopsie (METAVIR F4) - FibroScan (>14.6 kPa) - FibroTest score ≥0.75 und APRI >2 Nelson et al. Hepatol 2015;61(4):1127-1135. Woche 24 Ausschlusskriterien: - Vorherige Behandlung mit NS5A-Inhibitoren - Intoleranz vorheriger SOF + RBV Behandlung - HCC - Koinfektion mit HIV oder HBV ALLY-3 Studie: Hohe SVR12-Raten bei GT-3 Patienten ohne Zirrhose Overall 100 97 96 Treatment-experienced 94 69 58 63 80 SVR12, %a Treatment-naive 60 40 20 0 105 109 20 32 Absent Present 73 75 11 19 Absent Present 32 34 9 13 Absent Present Cirrhosis b,c • • 12 Wochen SOF + DCV hohe Heilungsraten bei nicht-zirrhotischen GT-3 Patienten Niedrige SVR12-Raten bei Zirrhose Patienten früher behandeln SVR12 defined as HCV RNA levels <LLOQ of 25 IU/mLa, either detectable or undetectable, at posttreatment Week 12 Assessed using the Roche HCV COBAS TaqMan Test v2.0 (LLOQ 25 IU/mL). Among patients with cirrhosis, 34% (11/32) had baseline platelet counts < 100,000/mm3; a HCV RNA <LLOQ (25 IU/mL), detectable or undetectable; error bars reflect 95% Confidence Intervals (CI).bCirrhosis status determined in 141 patients by liver biopsy (METAVIR F4), FibroScan (> 14.6 kPa), or FibroTest score ≥ 0.75 and APRI (aspartate aminotransferase to platelet ratio index) > 2.c Cirrhosis status for 11 patients was missing or inconclusive (FibroTest score > 0.48 to < 0.75 or APRI > 1 to ≤ 2).DCV, daclatasvir; SOF, sofosbuvir; SVR12, sustained virologic response at posttreatment week 12. ALLY-3: Safety & Resistenzanalyse • Gutes Verträglichkeitsprofil (1 SAE) • Häufigste unerwünschte Ereignisse: Kopfschmerzen (20%), Fatigue (19%), Übelkeit (12%), Durchfall (9%) • 10/14 Patienten mit NS5A-A30 Polymorphismus zu Baseline erreichten SVR12 • 7/13 Patienten mit NS5A-Y93H zu Baseline erreichten SVR12 • Keine Resistenz-assoziierten NS5B RAVs zu Baseline oder Relapse Modified according to Nelson DR, et al. Hepatol. 2015. 2015;61(4):1127-1135. ZUSAMMENFASSUNG: GT-3 Patienten ohne Zirrhose • Hohe Ansprechraten mit 12 Wochen DCV + SOF bei Patienten ohne Zirrhose • Bei GT-3 Patienten mit Zirrhose fallen die SVR12-Raten stark ab • Ungenügende Ansprechraten im Real-Life Setting bei SOF + RBV für 24 Wochen (TARGET Register) • Regime mit Interferon nicht mehr als Standardtherapie empfohlen EASL Empfehlungen für die Therapie der HCV Infektion bei Patienten ohne Leberzirrhose HCV-monoinfected or HCV/HIV coinfected patients with chronic HCV without cirrhosisa aTreatment-naïve patients and patients who failed a treatment based on PEG-IFNα +RBV GT, genotype; HCV, hepatitis C virus; PegIFN-α, pegylated interferon alfa; RBV, ribavirin. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol. 2015. doi:10.1016/j.jhep.2015.03.025. Kasuistik 1 Patienten-Informationen 39 jähriger Mann, ehemals iv-Drogenabhängig, seit 5 Jahren stabil substituiert (Methadon), selten Cannabiskonsum, therapienaiv, HCV Genotyp 3, F0/F1 Fibrose Bisher keine Therapie wegen Angst vor Nebenwirkungen Patient wünscht dringend Therapie (neue HCV negative Partnerin) Begleiterkrankungen / Komplikationen: Chronische Bronchitis Nikotinabusus Selten Cannabiskonsum Selten Alkohol Behandlungsvorschlag: 12 Wochen DCV/SOF aufgrund von ALLY-3 Daten (97% SVR12) gemäß Fachinformation DCV und Leitlinienempfehlung Herausforderung GT-3 und Zirrhose: Welche weiteren Studien und Daten gibt es? ALLY-1: DCV + SOF + RBV über 12 Wochen bei GT-3 Patienten mit Zirrhose Advanced cirrhosis cohort n = 60 100 SVR12 (% patients) 100 100 80 80 76 83 60 40 20 26 34 11 11 4 5 5 6 4 4 0 0 1a 1b 2 3 4 6 0 HCV Genotype • • Ribavirin verbessert die SVR12 Raten bei GT-3 Patienten mit Zirrhose Fachinformation DCV + SOF +/- RBV für 24 Wochen bei zirrhotischen GT-3 Patienten Modifiziert nach Poordad F, et al. Hepatology. 2016. doi: 10.1002/hep.28446 Compassionate Use Programm CUP (AI444-237): Daclatasvir Härtefallprogramm in Deutschland und Europa Beschreibung: • Härtefallprogramm von Daclatasvir in Deutschland im April 2014 durch das Bundesinstitut für Arzneimittel und Medizinprodukte (BfARM) genehmigt, um Patienten vor Marktzulassung den Zugang zu Daclatasvir zu ermöglichen1 • Nur Patienten mit chronischer HCV-Infektion und hohem Dekompensationsoder Mortalitätsrisiko innerhalb von 12 Monaten • Nur Patienten ohne alternative Therapieoption Methode: • rein deskriptive Analyse • open-label Daclatasvir 60 mg kombiniert mit Sofosbuvir 400 mg 1 x täglich über 24 Wochen modifiziert nach Härtefallprogramm / Compassionate Use, http://www.bfarm.de/DE/Arzneimittel/zul/klinPr/compUse/_node.html; Zugriff 13.4.15 European Multicenter Compassionate Use Program (AI444-237, Härtefallprogramm) – Behandlungsprotokoll1 Tag 1 Woche 24 Daclatasvir + Sofosbuvir ± Ribavirin 1x täglich*) Woche 36 Follow-Up Woche 72 Zusätzliches optionales Follow-Up SVR12 N = 482 Woche 48 SVR24 Zusätzliche Gabe von Ribavirin nach Ermessen des Arztes • Primäres Ziel Patienten mit chronischer HCV-Infektion und hohem Dekompensations- oder Mortalitätsrisiko den Zugang zur Therapie mit Daclatasvir ermöglichen, die keine andere Therapieoption zum aktuellen Zeitpunkt hatten • Patienten Mit weit fortgeschrittener Lebererkrankung, d. h. mit einem hohen Risiko für eine Leberdekompensation oder Tod innerhalb von 12 Monaten * Dosisanpassungen von Daclatasvir erlaubt für Patienten mit gleichzeitiger antiretroviraler Therapie; Welzel et al. Daclatasvir plus Sofosbuvir with or without ribavirin for the treatment of HCV in patients with severe liver disease: Interim results of a multicenter compassionate use program. J Hepatol 2015; 62: S619, P0772 Härtefallprogramm: Auswertung der GT-3 Population All Treated Patients N = 485 Excluded from this interim analysis, N = 20a • Did not reach posttreatment Week 12, n = 7 • Missing data (not caused by death or treatment discontinuation due to AE), n = 13 • Safety Population N = 102 All Treated GT 3-Infected Patients N = 102 Efficacy Population N = 82 Primary Efficacy Analysis (mITT): Patients with missing data who died, discontinued treatment due to AEs, or had virologic breakthrough/relapse before posttreatment Week 12 were classified as failures • Safety Analysis: Clinical (AEs, serious AEs, AEs leading to discontinuation, and deaths) and laboratory abnormalities a All patients had HCV RNA < LLOQ, TD or TND, at EOT (Week 24) or at the last available assessment. 1. Pol S, et al. Liver Intl 2014;34:(18–23); 2. Nelson D, et al. Hepatology; 2015;61(4):1127–1135; 3. EU CUP, AI444-237; ClinicalTrials.gov identifier NCT02097966. Härtefallprogramm bei Patienten mit weit fortgeschrittener Lebererkrankung: Wirksamkeit bei GT-3 – SVR12 (mITT) 86 88 87 80 DCV + SOF % ± 95% CI HCV RNA < LLOQ, TD or TND 100 60 DCV + SOF + RBV 40 All Patients 20 42 49 29 33 71 82 7 4 11 Breakthrough 1 0 1 Relapse 3 3 6 Discontinuation (AE) 0 1 1 Deatha 3 0 3 0 Not Achieving SVR12 Breakthrough: confirmed on-treatment HCV RNA ≥ 1 log10 IU/mL over nadir, or ≥ LLOQ if previously < LLOQ, TD or TND; Relapse: confirmed HCV RNA ≥ LLOQ during any posttreatment visit following HCV RNA < LLOQ, TD or TND, at end-of-treatment; a Includes 1 patient who died during follow-up period; HCV RNA < LLOQ at post-treatment Week 10. 1. Pol S, et al. Liver Intl 2014;34:(18–23); 2. Nelson D, et al. Hepatology; 2015;61(4):1127–1135; 3. EU CUP, AI444-237; ClinicalTrials.gov identifier NCT02097966. ZUSAMMENFASSUNG: GT-3 Patienten mit Zirrhose • Gute Ansprechraten mit 12 Wochen DCV + SOF + RBV in der Ally-1 Studie • Hohe Ansprechraten mit 24 Wochen DCV + SOF ± RBV im Compassionate Use Programm • Regime mit Interferon nicht mehr als Standardtherapie empfohlen EASL Empfehlungen für die Therapie der HCV Infektion bei Patienten mit Leberzirrhose HCV-monoinfected or HCV/HIV coinfected patients with chronic HCV with compensated (CP-A) cirrhosisa aTreatment-naïve patients and patients who failed a treatment based on PEG-IFNα +RBV CP-A, Child-Pugh Class A; GT, genotype; HCV, hepatitis C virus; PegIFN-α, pegylated interferon alfa; RBV, ribavirin. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol. 2015. doi:10.1016/j.jhep.2015.03.025. Kasuistik 2 Patienten-Informationen 53 jähriger Mann, Begleiterkrankung/Komplikationen: Depression portaler Hypertonus Aszites Z.n. Varizen 3. Grades Medikation: Spironolacton/Furosemid Propanolol Labor / Klinik HCV Genotyp 3 Bilirubin 4,3 mg/dl; Albumin 30 mg/dl; INR 1,6; Thrombozyten 75.000/μl; Kreatinin 1,5 mg/dl / GFR 40 ml/min; MELD 21 CHILD Pugh B Fibroscan 36,7 kPa = Leberzirrhose Klinisch stabil, Gelistet zur Leber-Tx Dringliche Indikation bei Zirrhose / HCC Risiko Behandlungsvorschlag: 24 Wochen DCV + SOF +/- RBV aufgrund von Härtefallprogramm Daten gemäß Fachinformation DCV und Leitlinienempfehlung. ZUSAMMENFASSUNG GT-3 Patienten und Therapie • schlechtere Prognose bei Patienten mit HCV GT-3 Infektion GT-3 Patienten mit hohem therapeutischem Bedarf • Heilung der HCV-Infektion (SVR12) verbessert Prognose generell HCV Patienten möglichst vor Auftreten einer Zirrhose behandeln • 24 Wochen SOF + RBV: keine optimale Option für GT-3 Patienten • 12 Wochen DCV + SOF: SVR12 über 90% bei GT-3 Patienten ohne Zirrhose • 24 Wochen DCV + SOF ± RBV: Hohe Heilungsraten bei GT-3 Patienten mit Zirrhose