und die Lunge wird immer schlechter… Cortison bei Alveolitis?
Werbung

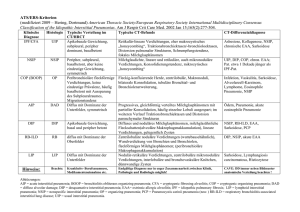
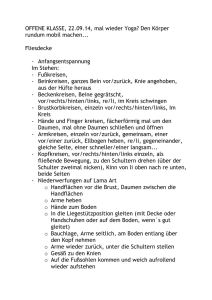
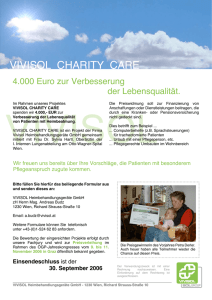
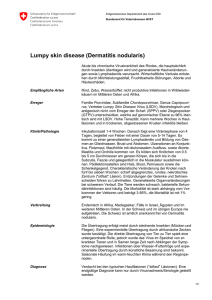
Kein Keim – und die Lunge wird immer schlechter… Cortison bei Alveolitis? OA Dr. Markus Stein RCU – Pneumolog. Abt. LKH Natters Leiter Primar Herbert Jamnig IFIMP, 19.06.2013 Infiltrat Infiltrat • Pat w, 43 a • Fieber, Leuko 20.000, CRP34, PCT 7,3 • Hypoxisches Lungeversagen • Intubation • Streptokokkenpneumonie CAP Woodhead et al, Community-acquired pneumonia on the intensive care unit: secondary analysis of 17,869 cases in the ICNARC Case Mix Programme Database, Critical Care 2006, 10(Suppl 2):S1 Differentialdiagnosen VAP - Inzidenz Ibrahim EH et al, Chest 2001 VAP - Inzidenz • 5,4 pro 1000 invasiver Beatmungstage • 1,6 pro 1000 nichtinvasiver Beatmungstage • ohne Beatmung 0,6 pro 1000 Patiententage Kohlenberg A et al. Pneumonia associated with invasive and noninvasive ventilation: an analysis of the German nosocomial infection surveillance system database. Intensive Care Med 2010; 36: 971–978 Interstitielle Erkrankung American Journal of Respiratory and Critical Care Medicine, Vol. 165, No. 2 (2002), pp. 277-304 Interstitielle Erkrankung Interstitielle Erkrankung American Journal of Respiratory and Critical Care Medicine, Vol. 165, No. 2 (2002), pp. 277-304 Diagnostik Röntgen CT Ground glass opacity Crazy paving Patchy Consolidation Wann Bronchoskopie ? • VAP – Beginn empirische Antibiose nach Risiko¹ – BRSK¹ – Deeskalation nach Antibiogramm¹ – Keine geringere Mortalität, aber Deeskalation² • ILD – Nicht so häufig diagnostisch³ – Ausschluss Infektion und Tumor³ ¹ Guidelines ATS und Infectious Diseases Society of America ² Heyland et al ³ The role of BAL in diffuse parenchymal lung disease; Current opinion in Pulmonary Medicine 2005, 11(5):417-421 Komplikationen Bronchoskopie • Hypoxämie • Blutung (TBB, PSB) • Pneumothorax (TBB, PSB) • Fieber/Infiltrat (BAL) • Keimverschleppung Hypoxämie • Während und nach Bronchoskopie • Ursache – Hypoventilation durch Sedation – Ventilation-Perfusionsmissmatch durch partiellen Verschluss der Atemwege und häufiges Saugen – Entstehen von Arrhythmien • Katz et al, Arch Intern Med 1981; 141: 603-606 • Sättigung ≥ 90% • Jones et al, Chest 2001; 119: 1906-1909 Bronchiolo Alveoläre Lavage • Mittels CT BAL planen • Portionsweise instillieren von 100 – 300 ml NaCl 0,9% • Absaugen • BAL Schlauch BAL Günther et al, Klassifikation, Diagnostik und Therapie der idiopathischen interstitiellen Pneumonien, Deutsches Ärzteblatt/Jg.100/Heft 24 TBB (transbronchiale Biopsie) • Pneumothoraxrisiko mit 15% bei beatmeten Patienten erhöht – Pincus et al, Crit Care Med 1987; 15: 1136-1139 – O´Brien et al, Crit Care Med 1997; 225: 440-446 – Turner et al, Crit Care Med 1994; 22: 259-264 prospektiv • Mangelhafte Representation – TBB 59% versus OLB 94% – Burt et al, Ann Thorac Surg 1981; 32: 146-153 Patient 1 • 69 a, w • Langjährig Cortison bei Polyarthritis • Leuko 20,3 • CRP 15,52 • PCT 1,79 • Hodgkin, Bleomycin, Mediastinalbestrahlung Patient 1 • BRSK: lymphozytäre Alveolitis • Dg.: DILD (drug induced lung disease) DILD – drug induced lung disease • • • • • 1972: 19 Medikamente 2007: >350 Medikamente, Zahl steigend Pathophysiologie unklar Dosisbezogen (z.B. Bleomycin) Cofaktoren: zunehmendes Patientenalter, renale Dysfunktion, Strahlentherapie, O2 Therapie, andere zytotoxische Substanzen • DAD als Komplikation: Mortalität 50-100% Lung, Drug induced Disease, Ali Nawaz Khan, www.emedicine.com Patient 2 • 65 a, m • Marginalzell-Lymphom • PCTH 1996 (Bleomycin) • Rezidiv 2005 • Tc VHFli, Sedacorone • Protrahierte Pneumonie • Leuko 1,7 Patient 2 • PcP (pneumocystic jeruveci) Patient 3 • 44 a, m • SLE, Hepatitis B, THelferzellmangel • PneumokokkenPneumonie ML • Panzytopenie • ANV • Prophylaxe mit TMPS, Valtrex, Diflucan Patient 3 • Am 5. Tag massive radiolog. Verschlechterung • Dg.: CMVPneumonitis • PCR 238:200.000 Open Lung Biopsy Baumann et al, Surgery Volume 143, Number 3, 426-433 Open Lung Biopsy Lettieri et al, Outcomes and safety of surgical lung biopsy for interstitial lung disease, Chest. 2005; 127(5):1600-1605 Open Lung Biopsy • Pulmonary hypertension, mechanical ventilation, and immunosuppressive therapy appear to increase the risk of death and other complications of surgical lung biopsy. Such patients are evaluated on a case-by-case basis to be sure that the procedure is likely to reveal a treatable diagnosis. Lettieri et al, Outcomes and safety of surgical lung biopsy for interstitial lung disease, Chest. 2005; 127(5):1600-1605 Labormarker • • • • • Leuko CRP PCT D Dimer, IL Antigen Streptokokken und Legionellen im Harn, Antikörper gegen Chlamydien und Mycoplasmen im Serum Procalcitonin Bloos et al, Multinational, observational study of procalcitonin in ICU patients with pneumonia requiring mechanical ventilation: a multicenter observational study. Critical Care 2011 15:R88 Procalcitonin Bloos et al, Multinational, observational study of procalcitonin in ICU patients with pneumonia requiring mechanical ventilation: a multicenter observational study. Critical Care 2011 15:R88 Therapie Therapie • COP Therapie • COP – Keine kontrollierten Studien – Therapieentscheidung basierend auf Guidelines, klinischer Erfahrung und Fallstudien • Bradley et al, Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63 Suppl 5:v1. Therapie • COP – Prednisolon – Optimale Dosis? – Initial 0,75-1 mg/kg IBW, bis 100 mg – Für 4-8 Wochen, dann langsam tapern • Bradley et al, Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63 Suppl 5:v1. Therapie • AIP früh spät AIP • • • • Ätiologie: unbekannt Fulminanter Verlauf, oft bei bisher Gesunden Histologie: DAD (diffuse alveolar damage) CT: Ground glass und consolidation (92%), Traktionsbronchiektasen, Verdickung des bronchovaskulären Bündels und der Interlobärsepten (Johkoh et al.; Radiology 1999), selten Honeycombing (Ichikado et al.; Am J Roentgenol 1997) Therapie • AIP – Fallberichte – Prednisolon • High dose: 1 gr/d Methylprednislon über 3 d, 1 mg/kg IBW über 1 Monat, dann tapern, Beginn Tag 3,5 mean, 8/10 Survivors – Suh et al, Early intervention can improve clinical outcome of acute interstitial pneumonia. Chest. 2006;129(3):753. • Kein Benefit – Vourlekis JS, Brown KK, Cool CD , et al. Acute interstitial pneumonitis: case series and review of the literature. Medicine (Baltimore) 2000; 79 (6) 369-378 Therapie • AIP – Alternative Immunsupression (MTX etc.) nicht empfohlen – Keine Daten zu Makroliden, Statinen – LUTX als Ultima Ration in Einzelfällen – Mortalität > 50% Infiltrat Zusammenfassung • Herausforderung therapieresistentes Infiltrat: multidisziplinäres Vorgehen • Radiologe, Pathologe, Infektiologe, Kliniker • Therapie bei Ausschluss Infektion: Cortison – Beginn? – Höhe? – Dauer? Es ist alles sehr kompliziert Dr. phil. Fred Sinowatz, 1929-2008 A U F M E R K S A M K E I T D I E F Ü R D A N K E