**************i******************B******* ****** **\*** ** *r
Werbung

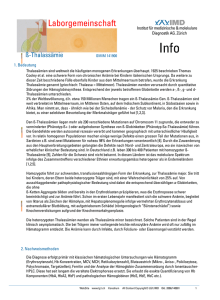
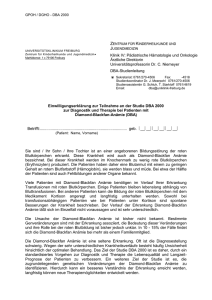
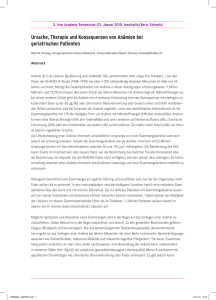
Eisenstoffwechsel und Anämietherapie: Neues von Eisen und Co. Prof. Dr. T. Frietsch 24.Nov 2012 0 med. Th. Frietsch, Vorsitzender der Interdisziplinären Arbeitsgemeinschaft für Klinische Hämotherapie IAKH e.V. Prof. Dr. Agenda • Anämie- und Eisentherapie - weshalb ? • Eisenstoffwechsel • Eisentherapie gestern und heute • Einbindung in praktische Konzepte 1 Präop. Anämie, Transfusion und Outcome Retrospektive Datenbankanalyse an 7759 Patienten Anämie Definition M: Hb < 13,5 g/dl; F: Hb < 12 g/dl Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology 2009; 110: 574–581. 2 13-02-01 9. Stuttgarter Intensivkongress Volumen- und Hämotherapie Beattie et al. Anesthesiology 2009; Maßnahmen 110: 574-81, Fremdblutsparende Ursachen der Anämie Ezekowitz et al. Circulation 107 (2): 223. (2003) iron deficiency 21% other deficiency 8% anemia of chronic disease 58% • Eisenmangelanämie: • Prävalenz in Europa: • Normalbevölkerung • Schwangere • Perioperativ • Intensivstation 3 othther identifiable causes 13% 6-10% bis 20% 20 – 30% ? , vmtl. > 50% Guralnik JM, et al. Blood. 2005;1:528-532. Prävalenz der periop. Anämie Ursache der Anämie Präop. Existent Referenz n Kollektiv Def. [Mean] [Hb in g/dl] Prä valenz Eisen- ACD mangel (EPO-M.) andere Guralnik et al.[1] 2 069 ohne 75 M13,0;F12,0 11% 20% 32% 34% Ezekowitz et al.[2] 12 065 Herzinsuff 77 k.A. 17% 21% 58% 21% Saleh et al.[3] 1 142 THA/TKA 68 M13,0;F11,5 20% 23%1 64%2 13% Bisbe et al.[4] 715 THA/TKA 68 M+F 13,0 19% 30%3 44% 26% Myers et al.[5] 225 THA 64 M12,5;F11,5 15% 60%4 34% 4% Basora et al.[6] 218 THA/TKA 71 M+F 13,0 39% 30% k.A.7 k.A. Theusinger et al.[7] 93 THA/TKA k.A. M13,0;F12,0 21%8 k.A. k.A. Goodnough et al.[8] 290 THA/TKA 60 57 M+F 13,0 30% 70%11 k.A. • 4 Alter 13-02-01 9. Stuttgarter Intensivkongress 21%9 33%10 J.Tomeczkowski, C. von Heymann 2011 unpublished Volumen- und Hämotherapie Beattie et al. Anesthesiology 2009; Maßnahmen 110: 574-81, Fremdblutsparende Die Anämie hat Auswirkungen auf – die Mortalität in der „Nichtherzchirurgie“ Retrospektive Datenbankanalyse bei 359 Patienten, Anämie Definition M: Hb < 13 g/dl; F: Hb < 12 g/dl Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology 2009; 110: 574–581. 5 13-02-01 9. Stuttgarter Intensivkongress Volumen- und Hämotherapie Gruson KI et al. J Orthop Trauma 2002; 16 (1): 39–44 Fremdblutsparende Maßnahmen Präoperative Anämie & Outcome Einfluss auf Mortalität und Morbidität Musallam KM, Kamam HM, Richards T et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study Lancet 2011; 378: 1396–1407. 6 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Epo und Fe als Anti-Anämika Nachteile blutgruppenkompatibler Erythrozytentransfusionen Kosten Verwechslung 1:10 000 Mortalität (Beatie) ? Infektionsrisiko (Bakterien, Hepatitis-, Zytomegalie- und Retroviren, PrionenCorwin HL et al for the EPO Critical Care Trials Group. “Efficacy and safety of Alzheimer) epoetin alfa in critically ill patients”. New Engl J Med 357: 965-76, 2007 TRALI Hypervolämie, TACO Elektrolytstörungen (Zitrat, K+, pH) Überladung des Organismus mit Eisen (Hämosiderose) Sensibilisierung gegen Histokompatibilitätsantigene Immunsuppression (Tumorrezidivhäufigkeit?) Versorgungsengpässe Hypothese: Epo/Fe-Therapie vermindert Ery-Transfusionsnotwendigkeit 7 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Patient Blood Management 8 Agenda • Anämie- und Eisentherapie - weshalb ? • Eisenstoffwechsel • Eisentherapie gestern und heute • Einbindung in praktische Konzepte 9 Eisenbedarf , Aufnahme und Verlust • • • • Bestand: Verteilung: 3-5 g / 70 kg Hämoglobin 66,1 % 2800 mg Depot-Eisen (Ferritin, Hämosiderin) 18,8 % 800 mg Nichthämenzym-Eisen 10 % 420 mg Myoglobin 4,7 % 200 mg Transport-Eisen (Transferrin) 0,2 % 10 mg Eisenhaltige Enzyme 0,2 % 10 mg Aufnahme: 10-15 mg / die, 10-15% Verfügbarkeit, Resorption 6-10%, Bei Mangel bis 20% Bedarf: Wachstum , Zellfunktion, Verlust Kollektiv Min Max Kleinkind 0,5 mg/die 1,5 mg/die Schwangere 2 mg/die 5 mg/die OP, Intensiv ? ? Epithelabschilferung- ca. 1 mg/die 100 ml Blutverlust: 50 mg Eisen ! (Menstruation 30-60 ml) 10 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Eisenstoffwechsel- Die Rolle von Hepcidin • Eisenzyklus: Aufnahme Duod. Cytoch. B Resorption ph Milz: MakrophagenAbbau Leber: Bindung an Transferrin Einbau in Epithel KM- Einbau in Erys Blutverlust • Abschilferung, Erneuerung Hepcidin: 1. Divalent metal transporter 1 ↓ 16-45% Plasma TSAT gesättigt - Resorption ↓ 2. Internalisierung und Degradation von Ferroportin 1 - Übernahme in Blut ↓ • 11 Eisenmangel: 13-02-23 Fe Ferritin Hepcidin Transferrin (Sättigung TSAT) Tfr Rez 1/2 ↓, → →, ↑ ↓ ↓ ↑ 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Eisen und Immunfunktion Recalcati S, Locati B, Cairo G Systemic and cellular consequences of macrophage control of iron metabolism Seminars in Immunology, Jan 15, epub ahead of print 12 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Eisen und (Herz-)Muskelfunktion Avni T, Leibovici L, Gafter-Gvili A Iron supplementation for the treatment of chronic heart failure and iron deficiency: systematic review and meta-analysis Eur J Heart Fail 2012; 14, 423-429 NYHA Class Anämie + Anämie - 13 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Pathophysiologie der periop. Anämie Perioperativ und bei Intensivpatienten • ist der EPO-Metabolismus verändert: 1. HIFa 2. EPO 3. Erythropoese - Transkriptionshemmung (TNFa, IL1b, IFNg, Neopterin) - Proliferation/Differenzierung - Apoptoseinduktion - Radikalbildung, NO, Superoxidanion • ist der Fe-Metabolismus verändert: 1. Hepcidin (IL6, TGFb, HIFa) FE-Freisetzung aus Speicher und intrazelluläre FE-Retention Ferritintranskription (TNFa, IL6, IL1b) Mucosablock Sing S, Gudzenko V, Fink MP. Pathophysiology of perioperative anaemia. Best Pract Res Clin Anaesth 2012; 26:431-39 14 13-02-01 9. Stuttgarter Intensivkongress Volumen- und Hämotherapie Beattie et al. Anesthesiology 2009; Maßnahmen 110: 574-81, Fremdblutsparende Therapie der Anämie Anämie bei chron. Erkrankung Funktioneller Eisenmangel + Anämie bei chron. Erkrankung 15 13-02-23 Latenter Eisenmangel Klassische Eisenmangelanämie http://www.labor28.de/laborinfo/labinfo145.html 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Eisensubstitution beim Intensivpatienten Lapointe M. Iron supplementation in the intensive care unit: when, how much, and by what route? Crit Care 2004; 8 Suppl 2: S37-41 16 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Agenda • Anämie- und Eisentherapie - weshalb ? • Eisenstoffwechsel • Eisentherapie gestern und heute • Einbindung in praktische Konzepte 17 Eisenpräparate 18 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Eigenschaften unterschiedlicher i.v. Eisenpräparate Eisengluconat 19 Molekulargewicht < 50 kD Komplexstabilität Eisensucrose Eisendextran (niedermolekular) Eisencarboxymaltose 34-60 kD 165 kD 150 kD gering mäßig hoch hoch akute Toxizität hoch mittel gering gering Maximaldosis 62,5 mg 500 mg 20 mg/kg KG 1.000 mg minimale Infusionsdauer 30 min 210 min 360 min 15 min maximale Einzeldosis bei Injektion 62,5 mg 200 mg 100 mg 500 mg maximale Injektionsdauer 10 min 10 min 2 min Bolus Testdosis erforderlich nein ja ja nein 13-02-01 9. Stuttgarter Intensivkongress modifiziert nach Gasche et al. Inflamm Bowel Dis 2007;13:1545–1553 Volumenund Hämotherapie Fremdblutsparende Maßnahmen Verträglichkeit der Fe- Carboxymaltose Lyseng-Williamson KA und Keating GM Ferric carboxymaltose: a review of its use in iron-deficiency anaemia Drugs 2009; 69:739-56 20 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Parenterales oder enterales Eisen ? Albaramki J, Hodson EM, Craig JC, et al. Parenteral verus oral iron therapy for adults and children with chronic kidney disease Cochrane Database Syst Rev 2012, CD007857 1 Intravenöses Hb- AnstiegEisen: • effektiver (Fe, TSAT, Hb) •EPO Dosis Ferritin Anstieg •Mortalität TSAT Anstieg •Kardiovaskuläre Morbidität EPO-Dosisreduktion •Gastrointestinal UW •Allergie, Hypotension 21 13-02-23 57. Jahrestagung der GTH München Favours IV iron Favours oral iron Eisenstoffwechsel und Anämietherapie Acta Oncol Downloaded from informahealthcare.com by UB Heidelberg on 01/29/13 For personal use only. IV Eisen bei Chemo-induzierter Anämie Figure 3. M eta-regression of total IV iron dose on log risk ratio for haematopoietic response. • Gafter-Gvill A, Rozen-Zvi B, Vidal L, et al. previously found to be a negative prognostic factor iron dose and haematopoietic response, suggesting in various malignancies, both solid and haematobetter response with a higher dose. T his is also in logical [27]. T he increase in haematopoietic response accordance with the anemiaresults of the Steensma et al. Intravenous iron supplementation for the treatment of chemotherapy-induced may be associated with better long-term overall trial [14,15], which is the largest trial included in the systematic review and meta-analysis ofit randomised controlled trials. survival. H owever, could not be assessed due to meta-analysis and the only trial that showed negative the short follow-up period of 15 to 18 weeks. results. T he planned iron dose was quite low (937.5 Intravenous iron for chemotherapy-induced anaemia 25 T he second fi nding of a 24% reduction in transmg) and the actual administered dose was even lower (650 mg) [29]. Acta Oncol 2013; 52:18-29fusion requirements is clinically important. Blood transfusions are associated with various risks as acute Trials differed in inclusion criteria regarding reaction, transfusion related acute lung injury, baseline iron parameter s. M ost trials excluded volume overload, and infections [4,13,28]. T herepatients with iron defi ciency. Of the nine trials that fore, reduction in transfusion requirement may reported baseline iron status, only two trials allowed minimise these risks. inclusion of true iron defi cient patients [24,26], but T he increase in haematopoietic response with IV their actual number in these trials was low. D espite iron was consistent in almost all settings, and was the differences in baseline iron status, meta-regresindependent of baseline iron status. M oreover, metasion demonstrated no association between baseline regression revealed a direct correlation between IV ferritin and T SAT and haematopoietic response. N=1681, 93% mit EPO Hb- Anstieg Zusammen oder ohne EPO effektiv Unabhängig vom Figure 2. I ntravenous iron vs. standard of care: Rate of patients who achieved a haematopoietic response. Black squares represent the point their sizes represent their weight in the pooled analysis, and the horizontal bars represent the 95% CI. T he black diamond at the Ausgangs-Eisenstatusestimate, bottom represents the pooled point estimate. CI, confi dence interval; IV, intravenous; RR, relative risk; ST D, standard. ahealthcare.com by UB Heidelberg on 01/29/13 ersonal use only. Mortalität und UWTransfusionsProfil vergleichbar vermeidung 22 13-02-23 [WM D 6.61 (95% CI 1.57, 11.65), random effects T here was no difference in the rate of any adverse model, fi ve trials]. event [RR 0.99 (95% CI 0.93, 1.04), four trials], adverse Five trials reported time to haematopoietic events that required discontinuation of iron [RR 1.01 response. Four trials repor ted time to response in (95% CI 0.59, 1.70), four trials], or serious adverse medians [11,23,25,26] and one reported in means events requiring intervention [RR 1.06 (95% CI 0.89, [24]. T he median time to response for the standard 1.27), seven trials]. In addition, there was no difference care group ranged between 46 and 94 days and the in the occurrence of thromboembolic events [RR 1.03 median time to response in the IV iron group ranged (95% CI 0.59, 1.80), four trials] or of cardiovascular between 36 and 54 days. events [RR 1.08 (95% CI 0.65, 1.78), six trials]. Six trials reported QOL outcomes. For the pooled analysis of QOL we included trials which repor ted the number of patients with an improvement in D iscussion FACT-Fatigue scale cantofincrease Figure 4. I ntravenous iron(a vs.clinically standard ofsignifi care: Rate patients who required blood transfusions. Black squares represent the point estimate, 57. Jahrestagung der GTH Eisenstoffwechsel und Anämietherapie Our systematic review compiles trials assessing was usually regarded a München 3 in point increase [22,25,26] their sizes represent theiras weight the pooled analysis, and the horizontal bars represent the 95% CI. T heall black diamond at theIV bottom Eisen bei gesteigerter Erythropoese Prospektive Kohorte , N=63, 3J Follow up Schlechteres Outcome mit: OR 4,89 OR 5,29 OR 0,89 iRF für Fe-Mangel: Phlebotomien Orale Antikoagulation 23 13-02-23 57. Jahrestagung der GTH München Überleben • NYHA >III • Eisenmangel • MCV ↓ KomplikationsFreie Zeit Van de Bruaene A, Delcroix M, Pasquet A, et al. Iron deficiency is associated with adverse outcome in Eisenmenger patients Eur Heart J 2011; 32, 2790–2799 Eisenstoffwechsel und Anämietherapie Agenda • Anämie- und Eisentherapie - weshalb ? • Eisenstoffwechsel • Eisentherapie gestern und heute • Einbindung in praktische Konzepte 24 Die Instrumente des PBM Optimierung der Hämatopoese •Anämie: Reduktion des Blutverlusts •Gerinnungsanamnese •Eigenblutspende •Beachte physiologische Reserven •Restriktiver Transfusionstrigger •Minimiere Blutverluste •Sorgfältige Blutstillung •Chirurgische Technik •Hämodilution •Cell Saver •Gerinnungsoptimierung •Optimiere HZV •Optimiere Sauerstoffversorgung •Restriktiver Transfusionstrigger •Achtsamkeit •Monitoring •Aufwärmen •Iatrogene Blutverluste ↓ •Gerinnungstherapie •Stressulkusprophylaxe •Infektionstherapie •Anämietoleranz •Anämietherapie •Sauerstoffverbrauch ↓ •Prompte Infekttherapie Diagnose und Behandlung •Planung Chirurgie •Anämiebehandlung: Eisen Erythropoetin 25 13-02-23 Postoperative Anämie 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Preop. anemia therapy is effective- a single center proof Kotze et al Effect of a patient blood management programme on preoperative anaemia, transfusion rate, and outcome after primary hip or knee arthroplasty: a quality improvement cycle. Brit J Anaesth 2012;108:943-52 • Prospekt. Anämietherapie nach Entwicklung eines Algorithmus anhand von retrospektiven Analysen • N = retro. 361 H, 356 K N = prosp. 155 H, 126 K • Intraop. Tranexamsäure, MAT und IHTN 26 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Preop. anemia therapy is effective- a single center proof Kotze A, Carter LA, Scally AJ. Effect of a patient blood management programme on preoperative anaemia, transfusion rate, and outcome after primary hip or knee arthroplasty: a quality improvement cycle Brit J Anaesth 2012;108:943-52 Anämieprävalenz: 24,3% vs 10,3% (vorher/nachher) Transfusionsbedarf , Wiederaufnahmerate LOS 0,7die/präop. mangelndem g HB Transfusionsbedarf 23% vs. 8% H, 7% vs. 0% K LOS 1die Wiederaufnahmerate um 3-5% 27 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Praktische Anwendung in ITS Heming N. et al. Iron deficiency in critical ill patients:...Crit Care 2011; 15: 210-17 •Therapeutisch auf der Intensivstation: Anämie < Hb 10-12 g/dl + • Therapie mit erwiesenem Transfusionsbedarf, z. B. ECMO • Intensiv-Therapiedauer > 5 Tage 28 • Inflammation und Sepsis nur EPO bis TSAT (<16%) Zusammenfassung • Eisenmangelanämie ist relevant für Outcome • Effektivität und Therapie der Anämie perioperativ derzeit von Evidenz (erste prospektive kontrollierte Studie (Kotze et al)) unterstützt • Vermutlich Kostenneutral durch – Komplikation, LOS, Transfusionsbedarf • EPO cave überschießend- Thrombosen ! • Fe cave Hämosiderose, Immunsuppression ? 29 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Danke für die Aufmerksamkeit 30 13-02-23 57. Jahrestagung der GTH München Eisenstoffwechsel und Anämietherapie Praktische Anwendung präop. Modell Damp (elektive Orthopädie- Implantatwechsel) ERYPO Nach FachInformation 600 I.E./kg KG zum Bsp.: 68kg KG = 40 000 I.E. (40K) 119kg KG= 40K + 30K 136kg KG= 40K + 40K Bei isoliertem Fe+ Mangel -3 Wochen p.o. 200 mg Fe-IISubstitution 31 pro Tag präoperativer Hb-Wert 10-11 g/dl Eisendiagnostik Ohne path. Befund Ziel 13g/dl -2 Wochen -1 Woche EPO s.c. +Fe i.v. OP OP EPO s.c. EPO s.c. +Fe p.o. /i.v. +Fe i.v. Bei normalem Fe+ -3 Wochen -2 Wochen präoperativer Hb-Wert 11-13 g/dl Eisen (TSAT) i.v. entsprechend Eisenmangel Diagnostik Var. Zusätze 85kg KG= 40K + 10K 102kg KG= 40K + 20K präoperativer Hb-Wert < 10 g/dl -1 Woche Ziel 14g/dl OP EPO s.c. EPO s.c. +Fe i.v.